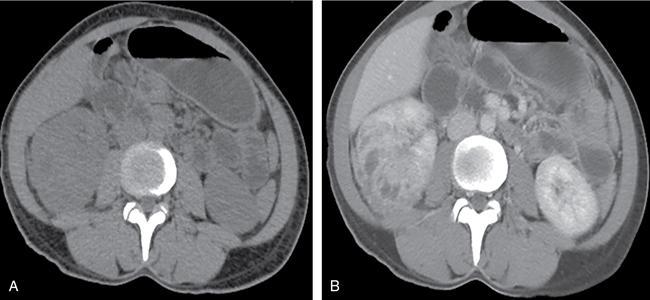
Renal fungal infections are rare, usually seen in immunocompromised patients and have increased mortality and morbidity. Many genitourinary fungal infections are confined to the bladder and urethra. Multiple imaging modalities aid in the primary diagnosis, follow-up and image-guided procedures. The most common causative pathogens are of the Candida species mainly Candida albicans, followed by Aspergillus spp., and Mucorales. Other fungi that have been described as causative pathogens include Rhizopus oryzae, Geotrichum candidu, Crypotoccci and Histoplasma. Pneumocystis jirovecii is implicated more commonly with retroviral disease. Renal fungal infections are rare, affect the neonates and elderly population. Common predisposing conditions include diabetes mellitus, urinary tract abnormalities, chronic indwelling catheters, immunocompromised state due to retroviral disease or postrenal transplant status, malignancy, prolonged antibiotic therapy, steroids and malnutrition. The pathogenesis of infection progresses through the phases of adherence, invasion of renal tissue, renal vascular invasion and subsequent dissemination. Complex infections can spread to the ureters and kidneys either through the haematogenous route or via ascending infection. Most patients are initially detected with candiduria, which develops into candidemia and disseminated candidiasis, thereby affecting the kidneys. Complex urinary infections are associated with fungal bezoars/balls/accretions results from aggregation of debris and necrotic tissue which are even rarer and may lead to obstructive uropathy. The fungal hyphae can aggressively invade the blood vessels, thereby leading to haemorrhage, thrombosis and infarction. This is most commonly seen in infections with Aspergillus and Mucor. Patients with renal fungal infection usually have systemic symptoms such as fever and can present as acute renal failure. Obstruction can cause diffuse abdominal pain or flank pain like a renal colic. With disseminated disease, features of sepsis set in. All patients with candiduria and underlying predisposing risk factors as mentioned before have to be carefully evaluated. Persistent candiduria in high-risk individuals should always prompt radiologic imaging of the kidneys and upper urinary tract with ultrasound or CT. On imaging, the commonly seen findings include initial renal microabscesses (parenchymal or subcapsular) which can progress to larger abscesses. Advanced disease leads to parenchymal necrosis and renal infarction. Fungal balls are also seen. Chronic and indolent infections may cause parenchymal calcifications. Though obsolete, conventional plain radiograph can demonstrate enlarged renal shadows with radiolucent fungal balls. On IVU, there may be nonvisualization of the affected kidney or delayed contrast excretion; and the fungal debris appears as filling defects within the opacified pelvicalyceal system. Secondary hydronephrosis due to obstruction by fungal ball may be seen. Unilateral renal involvement predominates over bilateral involvement. The affected kidney may appear bulky with indistinct corticomedullary differentiation. Presence of multiple small anechoic cystic foci with or without posterior acoustic enhancement areas represents microabscesses. Layered renal pelvic and calyceal wall thickening is seen with innermost hyperechoic rim representing the injured mucosal, central hypoechoic area represent submucosal oedema and infiltration and outermost thickest hyperechoic layer of muscularis. This layered arrangement of wall thickening is indefinitive sonological finding and is seen with other forms of pyelitis. On colour Doppler, peripelvic region and renal sinus may show increased vascularity. With progression of infection, the papilla is involved causing papillitis and resultant papillary necrosis, which serves as the nidus for fungal ball formation. Echogenic debris within a dilated pelvicalyceal system and ureter may be seen in early fungus ball formation. A fungal ball is seen as a mobile, echogenic, avascular mass with no posterior acoustic shadow in the renal pelvis, causing obstruction and hydronephrosis. Mobile intraluminal echogenic avascular mass with associated renal pelvic wall thickening favours an ongoing inflammatory process as opposed to a neoplasm. Associated renal arterial or venous thrombosis may be seen especially in invasive fungal infections. Interval follow-up with ultrasound should be done to look for the dissolution of the fungal ball, renal size, parenchymal echogenicity and grade of obstruction of the pelvicalyceal system. Globular enlargement of kidneys with reduced perfusion is visualized as poor heterogeneous contrast enhancement (salt and pepper appearance). Microabscesses are seen as small hypoattenuating parenchymal or subcapsular lesions (Fig. 10.12.2.8.1). Fungal balls are seen as rounded, heterogeneous soft-tissue attenuation lesions with variable contrast enhancement. They do not show any attachment to the walls of the urinary tract and are seen as filling defects on the excretory phase of CT urogram.
8. Renal fungal disease: Includes candidiasis and mucormycosis
Introduction
Epidemiology
Etiopathogenesis
Clinical features
Lab parameters
Imaging features
Plain radiograph and IVU
Ultrasonography
Computed tomography
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


