Malakoplakia is a chronic granulomatous multisystemic disease characterized by the presence of one or more white plaques in various organs of the body, preceded by chronic bacterial infection. In most of the reported cases, it was found that E. coli contributes to 80%. Malakoplakia originates from the Greek words, malakos (plaque) and pakos (soft). Malakoplakia affects many organ systems including gastrointestinal tract, lungs, bone, skin and lymph nodes. The urinary tract is frequently involved and all parts of urinary tract can be affected while the second most common site is kidneys. Patients with this pathology may be asymptomatic or show nonspecific symptoms, such as fever, pain, haematuria, renal failure and persistent UTI. The prevalence is unknown. It occurs predominantly in the female sex, with a ratio of 4:1 and the average age of diagnosis is at 50 years. It rarely occurs in paediatric ages. Most commonly seen in immunocompromised patients about 40%, which include posttransplant HIV/AIDS, lymphoma, poorly controlled diabetes, steroid therapy or alcoholism. With regard to urinary tract involvement, in 64% of cases the disease will affect both kidneys. Gram-negative bacteria are frequently associated with malakoplakia with E. coli found in at least two-thirds of lesions. In addition to this microorganism, other possible ones are described, such as Klebsiella, Proteus, Mycobacterium, Staphylococcus and fungi, which release cytokines and produce inflammation and kidney damage. Michaelis-Gutmann bodies are pathognomonic for the disease. They differentiate it from two similar processes which are megalocytic interstitial nephritis and XGP which lack the characteristic intense periodic acid-Schiff staining. Since malakoplakia commonly manifests as mucosal mass involving the ureter or bladder, the most frequent renal finding is obstruction secondary to lesion in the lower urinary tract. Usually normal. In later stage parenchymal calcification in renal shadow region. In excretory urography, filling defects can be observed in the collecting system. At US, malakoplakia lesions are typically described as poorly defined, hypoechoic masses seen within an enlarged, deformed kidney with distortion of the central echo complex. In computed tomography images, masses with heterogeneous enhancement of the contrast medium could be observed, which make it difficult to differentiate between acute infectious processes. Decreased excretion of contrast is more pronounced in cases with extensive parenchymal involvement. Parenchymal calcification is rare. Perinephric extension and renal vein thrombosis have been reported. MRI of malakoplakia lesions have depicted a relatively specific pattern of multiple 1–2-cm nodules with low signal intensity on T1- and T2-weighted images and delayed enhancement of intervening fibrous stroma. Unifocal renal lesion is uncommon and can resemble a renal cell carcinoma. Neovascularity is generally absent but can be seen with unifocal disease. Increased uptake of fluorodeoxy glucose was noted in the kidney on PET scanning. However, it is not a specific finding. Renal biopsy is the gold standard for diagnosis. The urothelium, which may be present, is superimposed, benign, and may be hyperplastic, metaplastic, or ulcerated, but is usually intact. The disease represents a rare granulomatous response to UTIs, usually; such response could be confused with malignancy, radiologically or endoscopically, and therefore in the literature this pathology is also known as pseudotumour.
7. Renal malakoplakia
Introduction
Clinical features
Risk factors
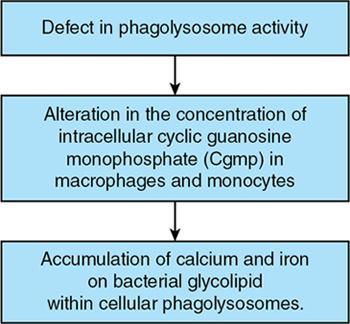
Pathogenesis
Pathology
Imaging features
Radiography
Excretory urography
Ultrasound
CT
MRI
PET
Renal biopsy
Differential diagnosis
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


