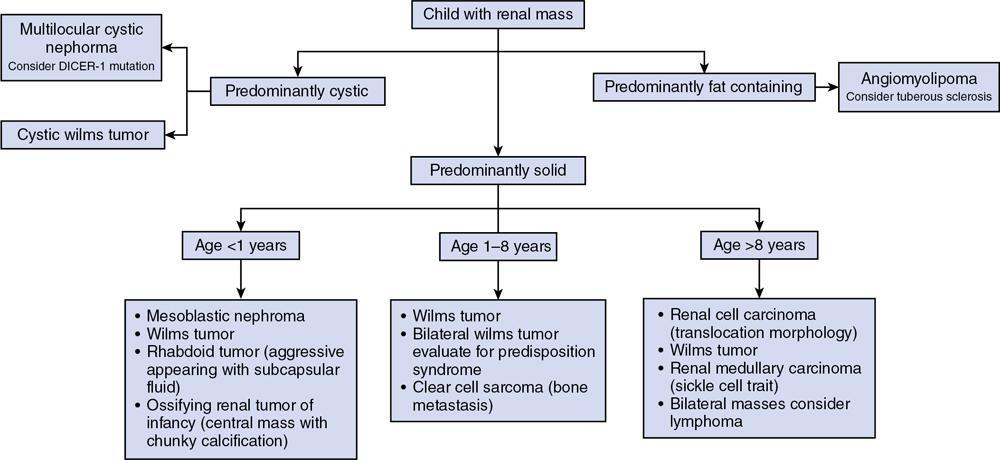
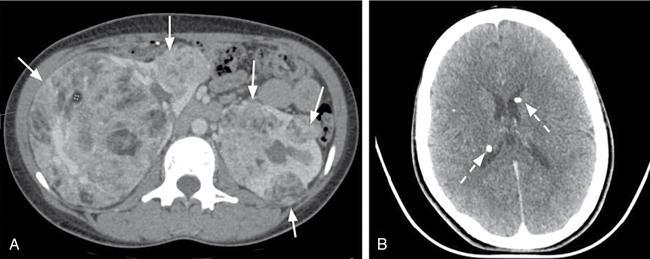
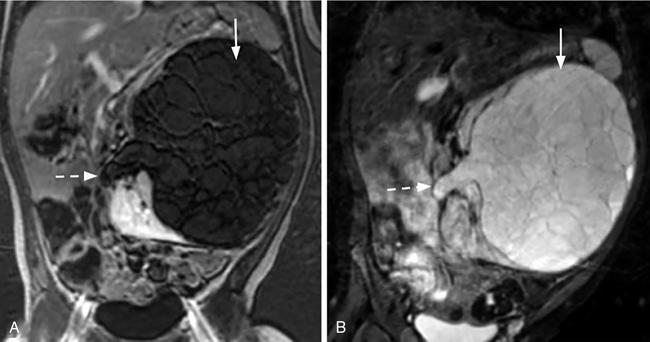
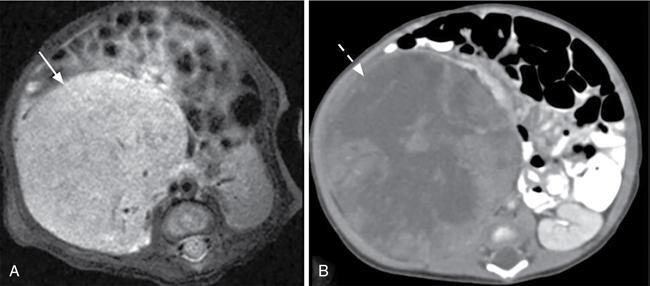
Naren Hemachandran, Devasenathipathy Kandasamy, Geetika Khanna Renal neoplasms are rare in children, accounting for less than 10% of childhood cancers. Nonneoplastic conditions like hydronephrosis, hypertrophied column of Bertin, foetal lobulations, calyceal diverticulum, simple renal cyst and infective causes like acute pyelonephritis, renal abscess can present as a renal mass clinically or on imaging. These nonneoplastic conditions are more common than true neoplasms in the early infantile period and radiologists should be aware of these conditions to avoid misdiagnosing them as neoplasms. In this chapter, we describe a clinic-radiological algorithmic approach as well as review the common paediatric renal neoplasms. Renal neoplasms can present as abdominal distension, mass palpable per abdomen (commonly detected by parents while bathing a child), flank pain, haematuria or rarely with other atypical symptoms. Imaging plays an important role in the detection, characterization, preoperative staging, image guided sampling, treatment planning and posttreatment follow-up or surveillance. Ultrasonography is the initial modality for detection as well as characterizing a mass as solid or cystic. This differentiation plays an important role in characterizing renal masses in children as further elaborated in this chapter. Computed Tomography (CT) is the preferred modality for further evaluation due to high spatial and temporal resolution and short scan times. In addition, CT allows for simultaneous evaluation for lung metastasis, a critical part of staging. Due to the need of sedation or general anaesthesia because of the longer acquisition time, Magnetic Resonance Imaging (MRI) is primarily used as a problem-solving tool and for evaluation of bilateral renal neoplasms. The characterization of renal masses in children may not always be possible by imaging due to significant overlap in the imaging and clinical features. In this chapter, we propose a radiological algorithm for the characterization of various renal masses in children. This is based on the primary nature of the mass and they are classified into predominantly fat containing, predominantly cystic and predominantly solid groups (Fig. 10.9.1). Predominantly solid masses are further subclassified based on the age at presentation. Various neoplasms have been categorized into these groups based on the most typical findings. This radiological algorithm is not absolute but intends to provide a practical approach to narrow down the differential diagnosis in a child with a renal mass. Angiomyolipoma is the most common fat-containing renal neoplasm in children. Other lesions like renal cell carcinoma, Wilms’ tumour also can show fat within. However, in such cases, fat component is seen along with other solid/cystic components and these do not present as predominantly fat containing and hence are described elsewhere. Angiomyolipomas are benign neoplasms and are composed of varying amounts of dysmorphic blood vessels, smooth muscle and fatty elements. In the adult population, the majority of them are sporadic, while the remaining 20% are seen in association with tuberous sclerosis. However, in children, the majority of the detected lesions are seen in association with tuberous sclerosis. The presentation varies with the size of the lesion. Small angiomyolipomas are typically detected during screening/annual surveillance of children with tuberous sclerosis. Those more than 4 cm are more likely to undergo spontaneous haemorrhage and present with pain, haematuria or rarely with life-threatening retroperitoneal or subcapsular haemorrhage. Although they are benign neoplasms, rarely they can show extension into the renal vein and subsequently into the inferior vena cava. On imaging, identification of a predominantly fat-containing mass enables us to confidently diagnose an angiomyolipoma (Fig. 10.9.2). However, there can be significant variation in the amount of fat within the lesion and some authors classify them into fat rich and fat poor angiomyolipomas. The fat can be either macroscopic fat or microscopic fat. The imaging features vary depending on the fat content. On ultrasonography, they are usually hyperechoic. The degree of heterogeneity of the lesion and the vascularity increases with increase in size of the lesion. Intratumoural prominent vessels, vascular lakes and pseudoaneurysms are well demonstrated on colour Doppler. CT is very helpful for the detection of the macroscopic fat even in smaller lesions. MRI helps in the demonstration of microscopic fat using chemical shift imaging, in which microscopic fat shows typical drop in signal intensity in opposed-phase images compared to in-phase images. Dixon technique is also very well suited for detection of small fat-containing angiomyolipomas, as the small foci of fat are very conspicuous on fat only images. The most common lesions that show predominant cystic areas on imaging are multilocular cystic nephroma, cystic partially differentiated nephroblastoma (CPDN)/cystic Wilms’ tumour. Previously these three tumours were considered to be along the same continuum with increasing blastemal components in CPDN compared to cystic nephroma, though recent studies have shown that these are distinct clinical/pathological entities. Multilocular cystic nephroma is a benign neoplasm more commonly seen in young boys. On sonography it appears as multiloculated cystic lesions with multiple thin septae within. The walls of the cyst and the septae show smooth thin enhancement on postcontrast imaging with no nodular or solid enhancing areas. The microcystic type can artifactually appear solid on imaging. These tumours typically present as Bosniak 3, and less commonly as Bosniak 2 renal cysts. Herniation into the collecting system is a characteristic finding, although it is not always seen (Fig. 10.9.3). Recent studies have shown a strong association of multilocular cystic nephroma with DICER-1 mutation. The lungs should be evaluated in these children for associated cystic lesions which can represent pleuropulmonary blastomas. The presence of solid enhancing component within a predominantly cystic lesion or nodular enhancement along the septae of a cystic lesion point towards a diagnosis of cystic Wilms’ tumour. Clinical, demographic features and the response to chemotherapeutic agents are similar to that of Wilms’ tumour, which is considered in detail in the next section. Most of the renal neoplasms in children are predominantly solid with significant overlap of imaging and clinical features. There are some typical features which are however, not seen always. We have further divided the predominantly solid masses based on the mean age of presentation of the lesions. This approach is not infallible, due to the wide range of the age of presentation of these lesions, and only aims to provide a practical working algorithm. Many times, even after the best of the efforts, it is impossible to pinpoint to a specific diagnosis and histopathology is needed to make the final diagnosis. Mesoblastic nephroma is the most common solid renal tumour in neonates. It was originally thought to represent congenital Wilms’ tumour. However, Bolande et al. in the late 1960s first described it as a separate entity and since then has been recognized as a distinct entity. It is also called as foetal renal hamartoma or leiomyomatous hamartoma. Mesoblastic nephroma typically presents in the first few months of life though it may be detected in utero on routine antenatal ultrasound or MRI studies. It shows a male preponderance. There are two histologic subtypes – classical and cellular types. The classical type shows features similar to that of uterine leiomyoma and is homogeneous with a whorled appearance. The cellular type tends to be larger, crosses the midline more often and occurs in slightly older patients (>3 months of age). Both the subtypes are unencapsulated but the cellular subtype shows a ‘pushing’ border with the adjacent kidney. The cellular type shows a multiseptated appearance with haemorrhage, necrosis and cystic areas resulting in a heterogeneous appearance (Fig. 10.9.4). Cellular mesoblastic nephroma tends to be more aggressive than classic. Calcification is rare and the absence of calcification is an important finding to differentiate it from the other common lesions seen in infants.
10.9: Renal masses in children
Introduction
Predominantly fat-containing masses
Angiomyolipoma
Predominantly cystic masses
Multilocular cystic nephroma
Cystic wilms’ tumour
Predominantly solid masses
Predominantly solid masses in <1 year of age
Mesoblastic nephroma
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


