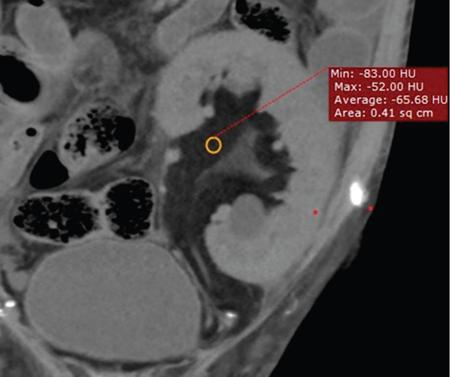
RRL is a more aggressive form of RSL usually occurring unilaterally. There is marked proliferation of fatty tissue within the renal sinus and hilum extending to the perirenal space. This occurs usually secondary to destruction or atrophy of renal parenchyma due to longstanding inflammation. This condition most commonly follows calculus disease and also has been associated with aging, renal TB and postrenal transplantation. As in RSL compensatory or inflammatory fatty proliferation secondary to renal loss are postulated as mechanisms of injury. It has been postulated that renal calculi trigger a process of hydronephrosis and chronic inflammation which in turn results in parenchymal atrophy and fibrofatty replacement in the sinus. Unlike RSL patients with RRL are usually symptomatic and present with recurrent flank pain, fever, and weight loss and mass per abdomen. RRL appears as a hyperechoic mass in the renal fossa often extending into the perinephric space. The kidney is often enlarged with atrophic parenchyma with or without visualization of a calculus. Helps make accurate diagnoses. It confirms the fatty nature of the pelvic lesion and differentiates it from nonfatty lesions of the pelvis (Fig. 10.12.2.6.2). CT scan defines the extent of the fatty proliferation in the renal fossa and in perinephric area, detects associated conditions such as hydronephrosis, renal/ureteric calculi and helps assessing the degree of parenchymal atrophy. Perirenal fat stranding and dilated, thick-walled and enhancing ureters have also been described.
Renal replacement lipomatosis (RRL)
Aetiology
Clinical signs and symptoms
Ultrasound
Computed tomography
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


