Fig. 1
Achilles tendinopathy
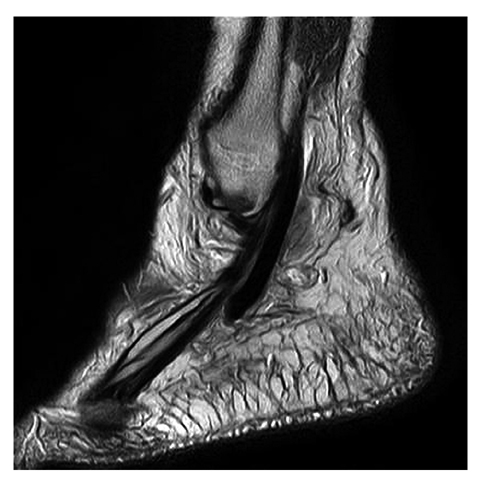
Fig. 2
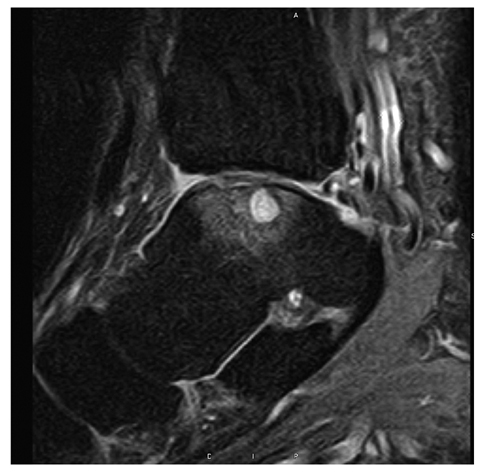
Longitudinal tear of the peroneus tendon
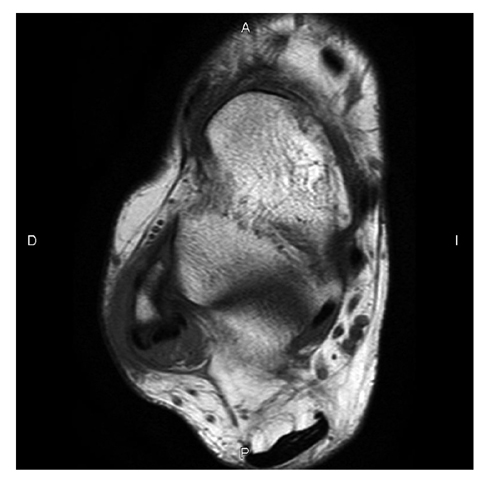
Fig. 3
Peronal splint syndrome
Tendon tearing can be thought of as predominantly a chronic process, with the „tear” being a culmination of long-standing disease. The degeneration may be silent but is nearly always present. Silent tendonopathy is more commonly fibrinoid (Fig. 4).

Fig. 4
Complete tear of the Achilles tendon
Achilles
Achilles disorders occur usually 2–3 cm from the insertion, and they often have visible, underlying degeneration, and they can be partial, interstitial or complete.
Older patients may have tears that are more proximal, and this is termed a myotendinous tear of the gastrocnemious.
Insertional tears may be seen in runners, or associated with rheumatoid or reactive arthritis. Haglund’s syndrome is seen distally, with a congenitally enlarge posterior tubercle, retrocalcaneal bursitis and insertional tendonosis (Fig. 5).

Fig. 5
Hadlund syndrome with partial tear of the Achilles tendon
Posterior Tibial
The posterior tibial tendon has two types of disorder. One type is seen around the malleolus; it is seen in older patients and is more common. Early stages of PTT disorder have associated synovitis, which is more often distal (Fig. 6).
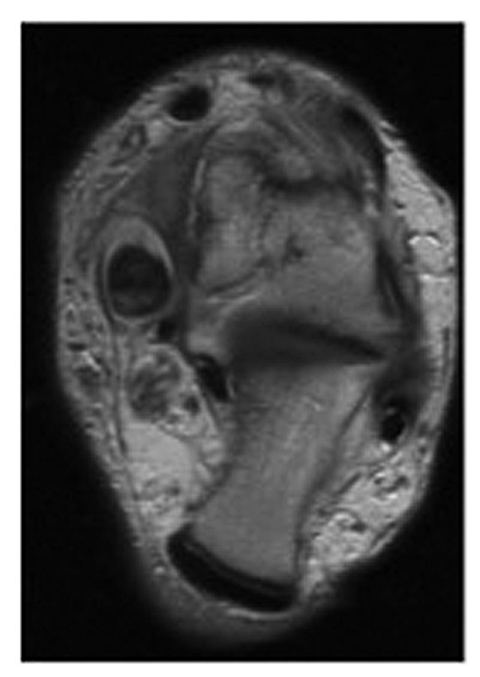
Fig. 6
Posterior tibialis tendinopathy
The second type of disorder is seen in young or active patients with seronegative or seropositive spondyloarthropathies. PTT disorders are manifest by a focally enlarged tendon, or less frequently a focal thinned tendon. Internal signal is less common.
Peroneus
Peroneal disorders include peroneal splits, which are interstitial tears often secondary to chronic subluxation long tears (Fig. 7). Relatively unique to the peroneal tendons, and also affecting the PTT, is tendon subluxation. This occurs because of a combination of biomechanical factors and anatomic factors such as a shallow groove. The splits that occur are often related to chronic instability of the brevis tendon. This can be related to ankle instability, or complex calcaneal fracture.
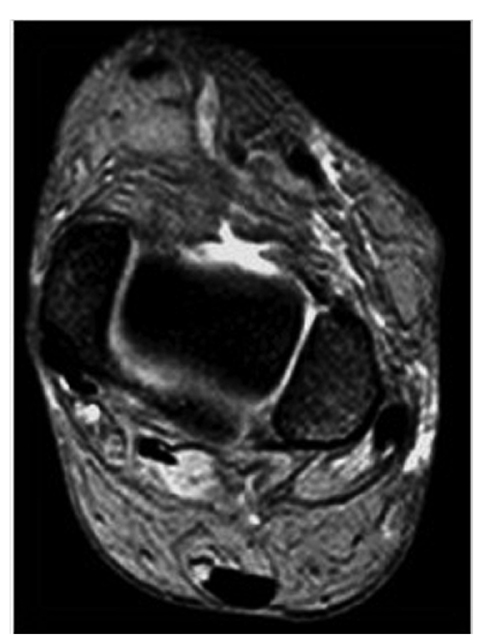
Fig. 7
Peroneal tendons subluxation
Anterior Tibial Tendon
Anterior tibial tendons can be clinically silent and can also be associated with arthropathies. These arthropathies include rheumatoid arthritis and gout. These tears are more often seen in the elderly, and very frequently are clinically silent [8].
Ligament Disorders
The most common ligament tear in the ankle is the anterior talofibular ligament (Fig. 8). It typically tears at its insertion onto the talus. The second most common is the calcaneofibular ligament, which also tends to tear distally, at its insertion onto the calcaneus. When acute, most of these tears demonstrate fluid violating the margins. On coronal images, the fluid dissects upwards in an anterior talofibular ligament injury and downwards in a calcaneo — fibular ligament injury The posterior talofibular ligament is rarely injured [9–11].
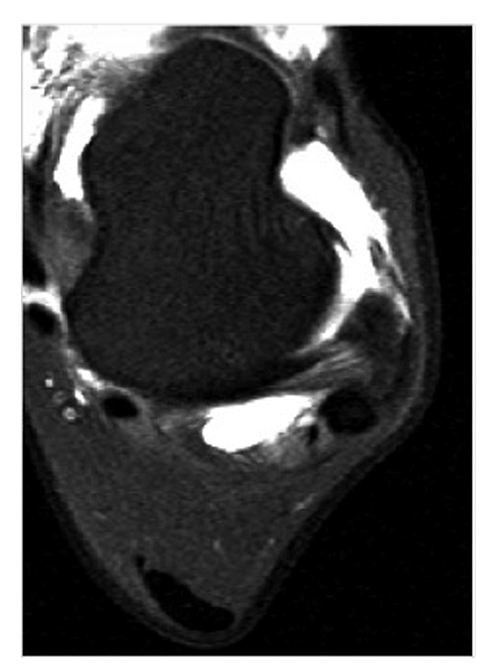
Fig. 8
Complete tear of the anterior talofibular ligament
Of somewhat more biomechanical importance are the syndesmotic ligaments. These are often associated with ankle joint instability. Asymmetry of the fibular within the sigmoid sulcus is a useful secondary sign, as is edema in the flexor hallucis muscle belly. Axial imaging for anterior syndesmotic ligament tears is difficult to interpret [12, 13].
Other Soft Tissues
The plantar fascia will degenerate in a similar way to tendon degeneration, as described above. When it tears, it tears approximately 5 mm from its insertion and demonstrates focal disruption. Tears may also be associated with muscle tearing, usually involving the flexor brevis or occasionally the quadratus plantae. Chronic disorders lead to a thickened fascia, with internal signal. Reactive marrow edema can also be seen in the calcaneus (Fig. 9). Reactive arthritis and rheumatoid arthritis can also lead to disruption of the plantar fascia [14, 15].
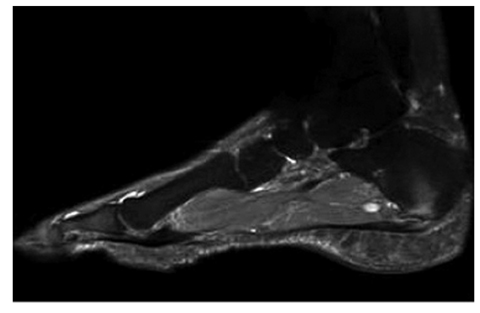
Fig. 9
Plantar fasciitis
Sinus tarsi syndrome is associated with ankle sprains and anthropathies of the subtalar joint. More useful than obliteration of the fat in the sinus is focal edema and disruption of the sinus tarsi ligaments; this should be clearly visible on most imaging protocols. Ganglia often extend laterally from the sinus tarsi, and marrow edema can be seen about the insertions of the ligament (Fig. 10).
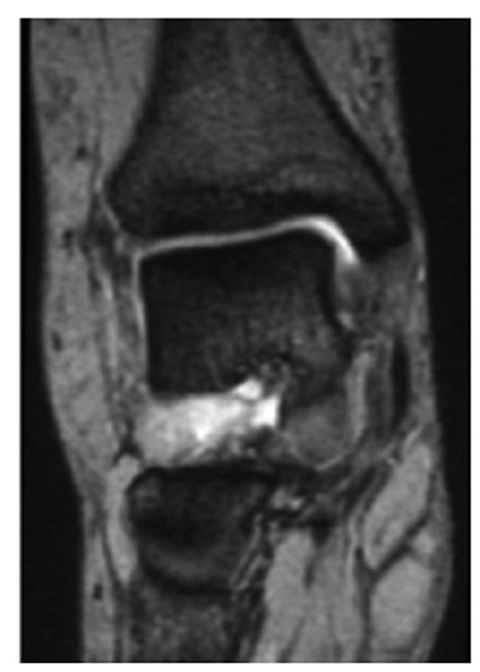
Fig. 10
Sinus tarsi syndrome
Tarsal tunnel syndrome is an infrequent indication for magnetic resonance (MR) imaging. Masses are disproportionately seen in tarsal tunnel syndrome, but still relatively uncommon. These masses include ganglia, varices, synovial cysts and ganglions [16].
Impingement syndromes of the ankle are chronic painful conditions secondary to repetitive friction between bones and soft tissue structures. They can be divided, following anatomic distribution, into: anterior, anterolateral, anteromedial and posterior impingement syndromes (Fig. 11). Anteromedial and anterolateral impingement syndromes are caused by hypertrophic synovial tissue and fibrosis, and MR arthrography might be helpful for accurate diagnosis [17].

Fig. 11
Anterior and posterior bone impingement
Bone Injuries
Marrow edema in the ankle has many causes, including osteochondral defects (Fig. 12), acute fractures, stress injuries and bone bruises; the latter are usually seen in association with ankle sprain, avascular necrosis and very rarely primary tumors, and rarely metastatic tumors [18–21]