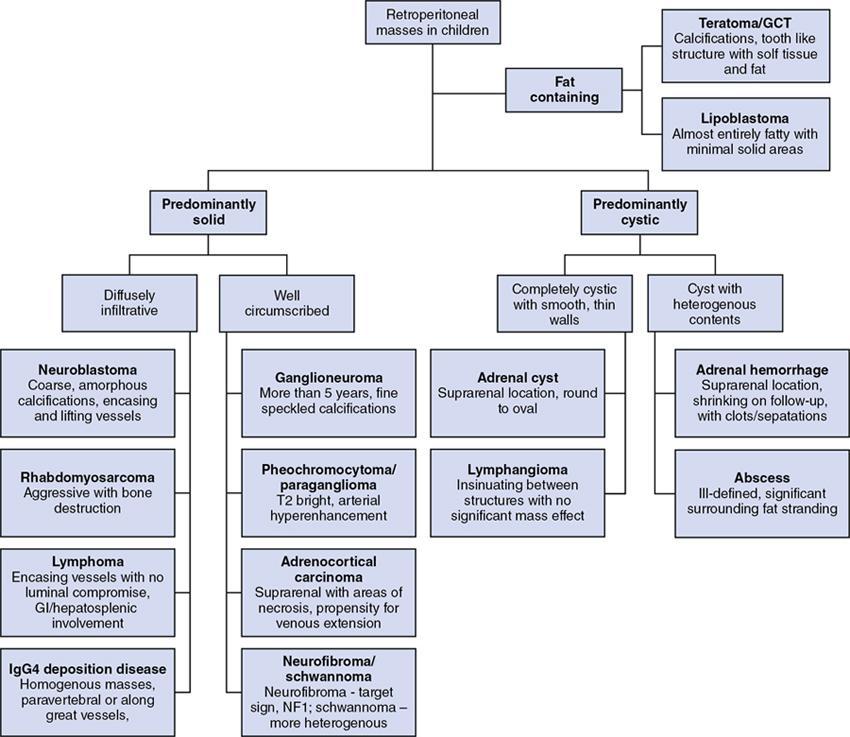
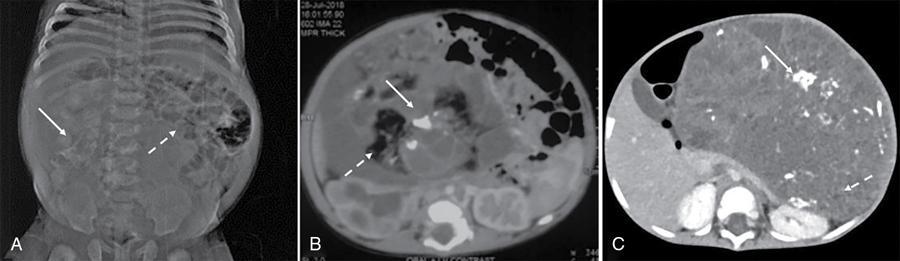
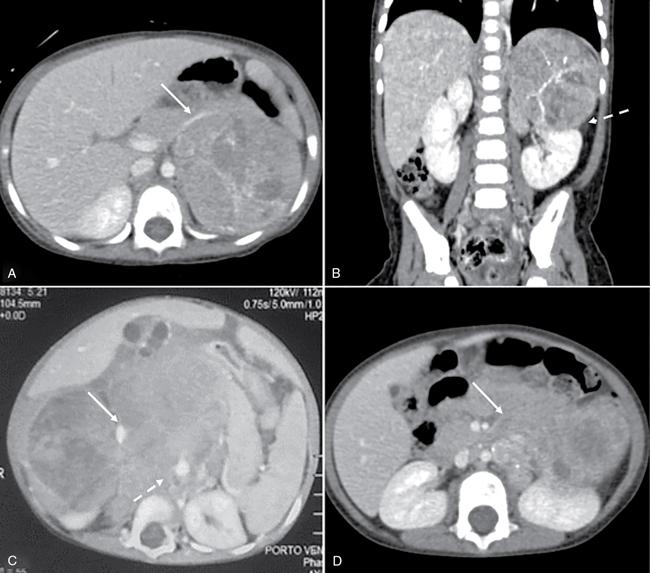
Devasenathipathy Kandasamy, Naren Hemachandran Retroperitoneal masses in children are relatively rare tumours and can primarily arise from the retroperitoneum or from any of the retroperitoneal organs (kidneys, adrenals, pancreas, duodenum, ascending and descending colon). This chapter primarily focuses on the primary retroperitoneal and adrenal masses. The spectrum of tumours affecting the paediatric age group is considerably different from those seen in the adults. The wide spectrum of diseases results in a wide range of clinical presentations which range from totally asymptomatic to even neurological symptoms in some. The presentation is usually nonspecific and imaging plays a major role in identification and characterization of these lesions. Ultrasonography is the initial modality used in children with any abdominal symptoms. Ultrasonography primarily serves three purposes. Firstly, as a screening tool for the detection of these masses, which would then be further evaluated with Computed Tomography (CT) or Magnetic Resonance Imaging (MRI), and secondly for characterizing whether a mass is cystic or solid and thirdly to localize it. CT is the workhorse in the evaluation, localization and characterization of retroperitoneal masses in children. Due to short scan times and a high spatial resolution, CT is the preferred modality in children with retroperitoneal masses. MRI in children usually requires deep sedation or general anaesthesia due to the longer acquisition time. Thus, in spite of a better contrast resolution, MRI is only used as a problem-solving tool. In this chapter, we propose a radiological algorithm for the characterization of various retroperitoneal masses in children. This is based on the primary nature of the mass and they are classified into fat containing, predominantly solid and predominantly cystic groups (Fig. 10.10.1). Various diseases have been categorized into these groups based on the most typical findings. Although not absolute, this radiological algorithm would provide a practical approach to narrow down the differential diagnosis in a child with a retroperitoneal mass. The identification of fat within a lesion considerably narrows down the differentials. The identification of intralesion fat is more easily accomplished on CT/MRI than on ultrasonography. The most common fat containing retroperitoneal lesions in a child are teratoma and lipoblastoma. Teratomas are usually complex solid cystic masses with fat and calcifications, while lipoblastomas are predominantly fat containing masses with variable amounts of enhancing soft tissue. Teratomas are the most common type of germ cell tumours in children. They can be mature, immature and mixed malignant types. Of these, benign mature teratomas are the most common and they show the presence of derivatives of all three embryonic layers – ectoderm, mesoderm and endoderm. They usually present as a painless increase in abdominal girth with a palpable abdominal lump. Imaging shows a heterogeneous solid-cystic mass with variable amount of fat and calcifications. The calcifications are coarse, chunky and well-formed bony components such as teeth are characteristic. Immature teratomas are larger, heterogeneous with or without significant fat component. Presence of haemorrhage or necrosis in a predominantly solid mass is suggestive of malignancy. Benign lesions show mass effect and displacement of the adjacent structures while invasion is typically seen in malignant ones. Other germ cell tumours are seminomatous and nonseminomatous germ cell tumours which include embryonal carcinoma, choriocarcinoma and yolk sac tumour. Primary retroperitoneal germ cell tumours (apart from teratomas) are very rare and majority of them are nodal deposits seen in a patient with a primary gonadal germ cell tumour. These are benign tumours of fatty origin (adipocytes) seen predominantly in infants and children. Lipoblastomas are well delineated, circumscribed, encapsulated lesions while lipoblastomatosis are unencapsulated locally invasive lesions. On imaging, they are almost entirely fatty with variable amounts of enhancing soft tissue components within. This group constitutes the most common retroperitoneal lesions in children. They can be subclassified into those that are diffusely infiltrative and those that are well circumscribed/encapsulated. The former includes neuroblastoma, rhabdomyosarcoma, lymphoma and IgG4 deposition disease while the latter includes ganglioneuroma, adrenocortical carcinoma, neurofibroma and phaeochromocytoma/paraganglioma. Neurogenic tumours can be classified into those of ganglion cell origin (sympathetic and parasympathetic) and those of nerve sheath origin. Tumours of sympathetic ganglion cell origin include ganglioneuroma, ganglioneuroblastoma and neuroblastoma in the increasing order of malignant potential. Tumours of nerve sheath origin can be benign or malignant. Benign nerve sheath tumours include neurofibroma and schwannoma, while their malignant counterpart is malignant peripheral nerve sheath tumour. Of these, neuroblastoma and ganglioneuroblastoma show overlapping clinical and radiological features and are described together here. Those lesions, which are the benign end of the spectrum (ganglioneuroma, schwannoma and neurofibroma), usually present as well-circumscribed lesions and are described in the next section. Neuroblastoma is the most common and the most malignant amongst the spectrum of neurogenic tumours of sympathetic ganglion cell origin. Overall, they represent the fourth most common paediatric malignancy after leukemia, CNS neoplasms and lymphoma. It is usually diagnosed below the age of 5 years (median age of diagnosis – around 16 months). Rarely they can also be diagnosed in-utero on ultrasonography or even in children above the age of 10 years. They can present with a wide range of symptoms and the degrees of symptoms are not related to the size of the tumour. The most common sites of origin of neuroblastoma are adrenal medulla (35%), primary retroperitoneum (30%) followed by posterior mediastinum (20%), pelvis/presacral space (2%–3%) and neck (1%–2%). Nearly half to two-thirds of the patients have disseminated disease at the time of diagnosis with metastasis to bone, liver, lymph nodes or skin. Primary multifocal neuroblastoma is rare and may be familial. They can be synchronous or metachronous noncontiguous tumours. On imaging, these are usually seen as large heterogeneous, diffusely infiltrative, lobulated masses with calcifications in nearly 90% of abdominal neuroblastomas. Heterogeneity is due to areas of necrosis and haemorrhage within the lesion. The lesion lacks a definite capsule and this accounts for its diffusely infiltrative nature, although relatively well-defined masses are not uncommon. Multiple large bulky nodes can be seen with characteristics similar to the primary tumour and this makes the differentiation of the tumour from the adjacent nodal mass difficult. There can be encasement of the vessels without luminal invasion. They typically insinuate around the major vessels and lift the aorta off the vertebral column. Adjacent organs like kidneys are usually displaced by the mass effect. However, they can also show direct invasion of adjacent organs and structures like psoas muscle. Intraspinal extension can be seen and is more often seen in thoracic neuroblastoma than with abdominal neuroblastoma. The International Neuroblastoma Staging System (INSS), first proposed in 1988 and modified in 1993, is still widely used (Table 10.10.1). However, it is based on the extent of tumour removal on surgery and hence cannot be used as a pretreatment staging system.
10.10: Retroperitoneal masses in children (including adrenals)
Introduction
Fat containing lesions (Fig. 10.10.2)
Teratomas
Lipoblastoma and lipoblastomatosis
Predominantly solid lesions
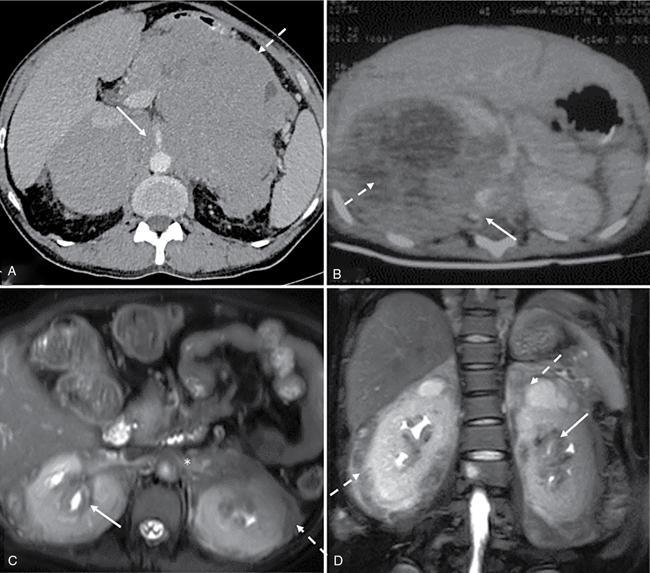
Predominantly solid lesions – diffusely infiltrative (Figs. 10.10.3 and 10.10.4)
Neuroblastoma
Radiology Key
Fastest Radiology Insight Engine