CROSS-SECTIONAL IMAGING ANATOMY OF THE RETROPERITONEUM
Tanvi Vaidya
Introduction
The retroperitoneum is a complex anatomical space, bordered anteriorly by the posterior parietal peritoneum and posteriorly by the transversalis fascia; extending superiorly from the diaphragm to the pelvic brim. It is composed of two lateral compartments and a central compartment; all of which are delineated by various fascial planes.
Each lateral compartment is further divided by the fasciae into three distinct spaces: (1) the anterior pararenal (APR), (2) perirenal and (3) posterior pararenal (PPR) spaces.
The central or vascular compartment is situated between the perirenal spaces, posterior to the anterior pararenal space and in front of the vertebral column.
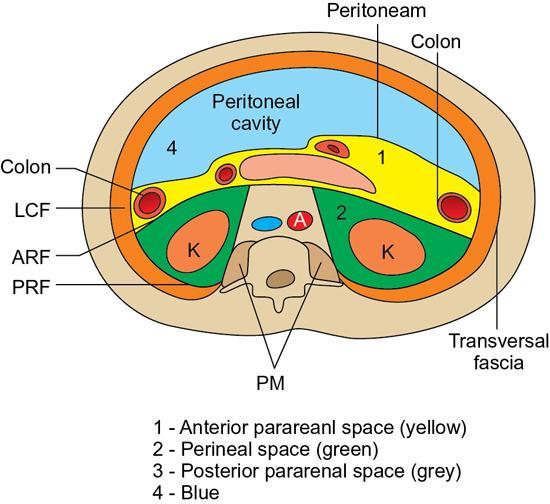
Boundaries, communication and extent: This space is located between the posterior parietal peritoneum anteriorly, the anterior renal fascia/Gerota’s fascia posteriorly and lateroconal fascia laterally. Medially it is potentially continuous across the midline, around the pancreas. Superiorly, the anterior pararenal space extends to the dome of diaphragm, just posterior to the intraabdominal segment of the oesophagus; and hence to the mediastinum, on the left and up to the inferior layer of the coronary ligament on the right. Inferiorly, the anterior and posterior pararenal spaces merge below the cone-shaped perinephric space, to form a common infrarenal compartment which communicates with the extraperitoneal spaces of the pelvis including the perivesical, prevesical and presacral spaces.
Contents: The anterior pararenal space contains the pancreas, duodenum, ascending and descending colonic segments, root of the small bowel mesentery and the transverse mesocolon. Owing to paucity of fat, delineation of this space may be difficult, unless it is distended due to fluid accumulation.
Applied anatomy: Inflammatory conditions such as pancreatitis, appendicitis and diverticulitis and resultant fluid collections such as pseudocysts and abscesses involve the anterior pararenal space (Fig. 10.17.1.3). Pancreatic pseudocysts could sometimes occur in the posterior mediastinum owing to its communication with the anterior pararenal space. Similarly, fluid collections related to appendicitis could extend into the pelvis.
2) The perirenal space
Boundaries, communication and extent: located between the anterior renal fascia and the posterior renal fascia, this space mainly contains the kidneys, suprarenal glands and renal vessels on either side. Laterally, it is limited by the lateroconal fascia formed by the fusion of the anterior and posterior renal fascia, posterior to the ascending and descending colon on either side. The lateroconal facia continues anteriorly to merge with the posterior peritoneal reflection thus forming the paracolic gutter on either side. Medially the anterior renal fascia with connective tissue that surrounds the great vessels in the central compartment while the posterior renal fascia fuses with the fascia of the psoas major or quadratus lumborum muscles. The perirenal spaces communicate across the midline via the Kneeland narrow channel located immediately anterior to the central/vascular compartment.
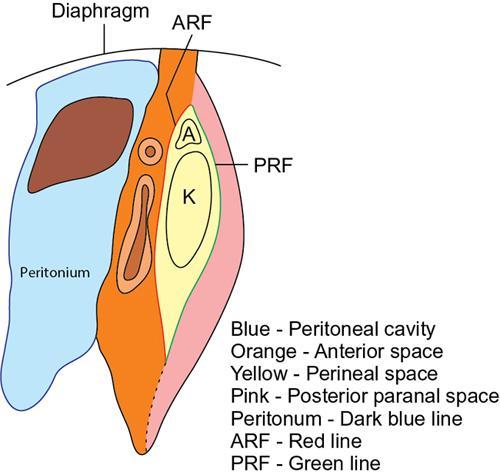
Superiorly the anterior renal fascia blends with the inferior coronary ligament on the right and with the gastrophrenic ligament on the left, while the posterior renal fascia fuses with the inferior phrenic fasciae bilaterally. Thus, the perirenal space is in continuity with the bare area of the liver on the right and the subphrenic space on the left and also communicates with mediastinum via the diaphragm hiatus and splanchnic foramina of the diaphragmatic crura.
Inferiorly the anterior and posterior renal fascia begin to converge below the inferior pole of the kidney lying in close contact with periureteric connective tissue however, do not fuse. The inferior cone of the perirenal space is open towards the iliac fossa, in contact with the psoas muscles, ureter and is continuous with prevesical and presacral spaces.
Contents: The perirenal space contains the kidneys, suprarenal glands, proximal ureters, perirenal fat, lymphatic vessels and renal vessels. The perirenal fat contains numerous bridging fibrous septae, which are of three types: (1) those extending between capsule and the anterior/posterior renal fascia, (2) those attached only to the renal capsule forming a curved arch and (3) those connecting the anterior and posterior renal fascia. These septa serve as supports for the kidneys; furthermore this may limit the spread of disease or serve as conduits for disease extension between the perirenal space and the renal fasciae (Fig. 10.17.1.4).
Applied anatomy: Blood from a ruptured abdominal aortic aneurysm may track into the perirenal space via the narrow channel across the midline. Haematomas or laceration involving the liver parenchyma or capsule adjacent to the bare area, can manifest with blood collection in the right pararenal space. Conversely right-sided perirenal haematomas or fluid collections could extend along the bare area of the liver. In addition, perirenal space collections may extend into the retroperitoneal space of the pelvis via the inferior communication/aperture.
3) The posterior pararenal space
Boundaries, communication and extent: located between the posterior renal fascia, anteriorly and the fascia transversalis, posteriorly. The space is limited medially by fusion of the posterior renal and transversalis fasciae with the muscular fasciae, adjacent to the psoas major with no communication across the midline. In its lateral aspect, continues as the properitoneal fat of the abdominal wall outer to the lateroconal fascia. It is this properitoneal fat which is visualized as the lucent flank stripe on plain abdominal radiographs. Inferiorly the posterior pararenal space is open to the pelvis and communicates with the prevesical space, femoral sheath, the anterior pararenal and perirenal spaces via the infrarenal space. The superior extent of the posterior pararenal space is determined by fusion of the posterior perirenal fascia with the fascia of the psoas and quadratus lumborum muscles and the inferior phrenic fascia. It generally continues as a thin layer of extraperitoneal fat in the subdiaphragmatic region.
Contents: The posterior pararenal space contains fat, blood vessels and lymphatics, but no major organs. Thus, involvement of this space by disease processes is usually due to extension from adjacent spaces/viscera (Fig. 10.17.1.5).
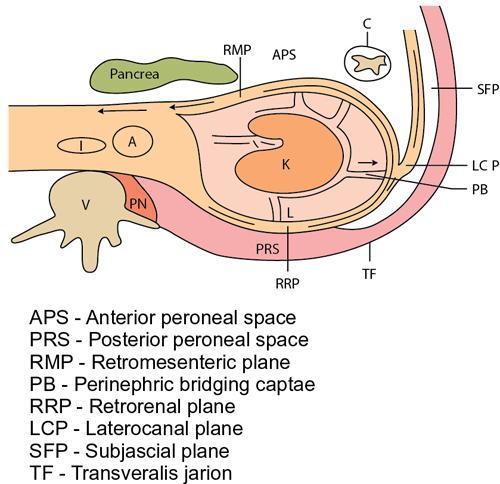
Fig. 10.17.1.1Schematic transverse section depicting the anatomy of the retroperitoneum and fascial planes: Lateral compartment: Anterior pararenal space, perirenal space, posterior pararenal space. Central/vascular compartment containing the great vessels.
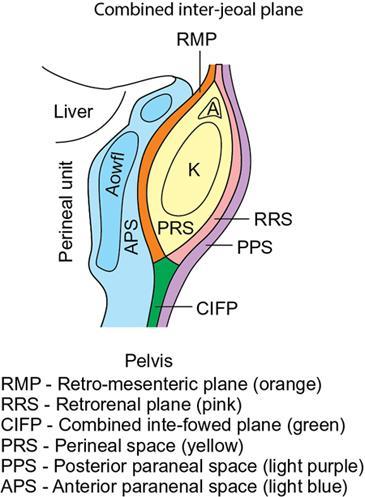
Fig. 10.17.1.2Schematic sagittal section depicting the anatomy of the retroperitoneum and fascial planes: Anatomy of the lateral compartment, extent and relationship of the retroperitoneal spaces.
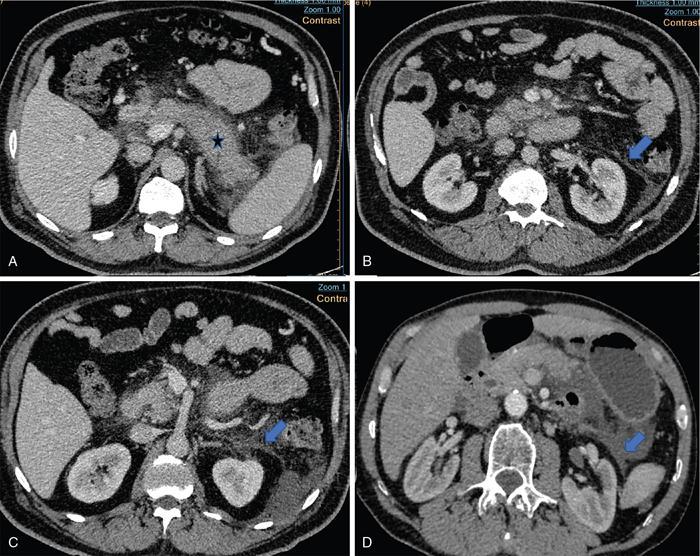
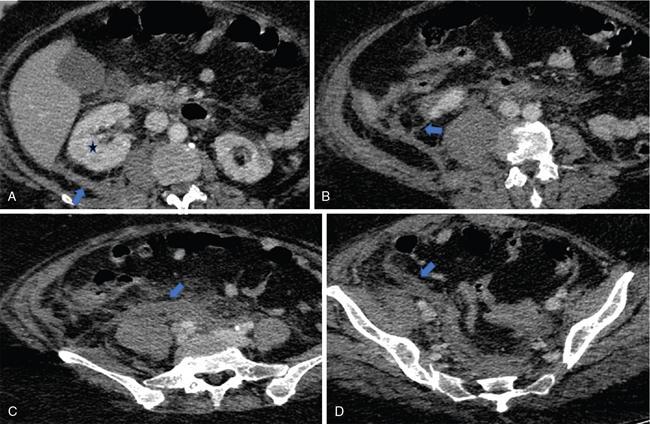
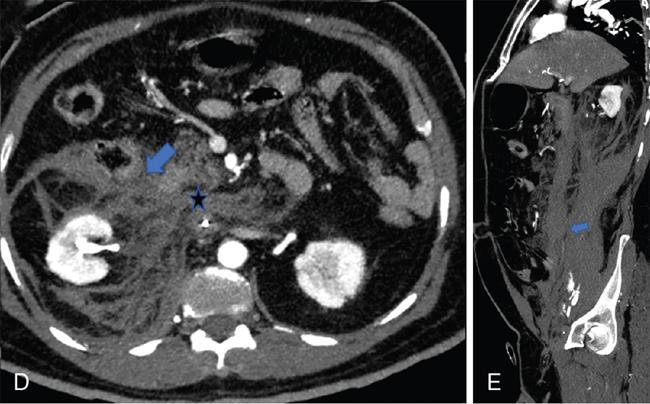
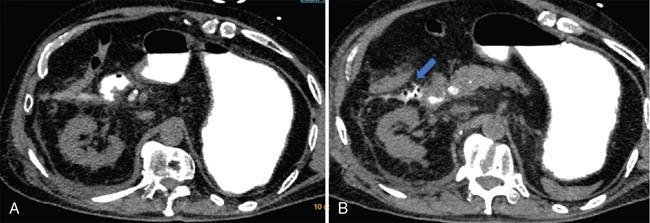
Fig. 10.17.1.3Contrast-enhanced axial CT sections in a case of acute pancreatitis (asterisk in A); the pancreas appears diffusely bulky with peripancreatic fat stranding. Thickening of the anterior renal fascia (blue arrows in B and C) with fluid collection in the anterior pararenal space (blue arrow in D).
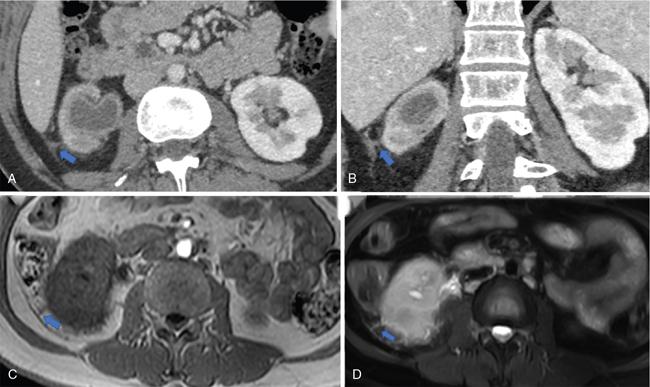
Fig. 10.17.1.4Contrast-enhanced axial and sagittal CT sections in a case of acute right pyelonephritis (A and B); the right kidney appears bulky with perinephric fat stranding. Thickening of the perinephric bridging septae (blue arrows in A and B) and posterior renal fascia. Axial T1W and axial STIR images also depict the thickened perinephric bridging septae (blue arrows in C and D).
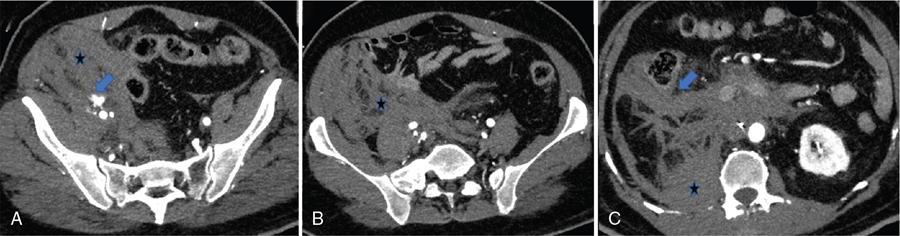
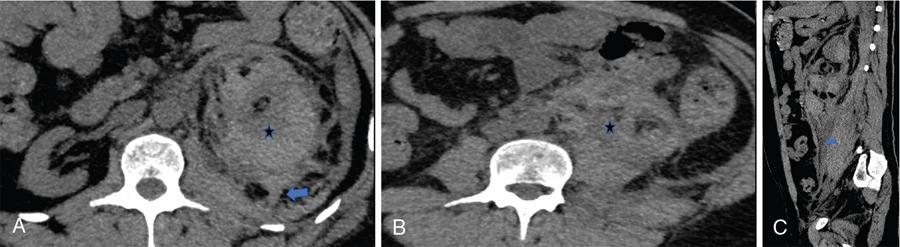
Fig. 10.17.1.5Contrast-enhanced axial CT sections in a case of acute right pyelonephritis (A–D); the right kidney appears bulky with perinephric fat stranding (asterisk in A). Thickening of the posterior renal fascia (blue arrow in A) and perinephric bridging septae (blue arrow in B). The inflammation extends into the right iliac fossa via the inferior cone of the perirenal space, in contact with the psoas major muscle (blue arrows in C and D).
Concept of retroperitoneal interfascial planes
The retroperitoneal fasciae are not composed of single-layered membranes, but are multilayered, thereby leading to the formation of potential, expansile fascial planes. These may serve as connecting channels for the spread of inflammatory or neoplastic conditions between the peritoneal, retroperitoneal and pelvic spaces. Alternatively, spread along these pathways could aid the decompression of large haematomas, fluid or gas collections in the abdomen.
The four fascial planes of the retroperitoneum include the retromesenteric, retrorenal, lateral conal and combined interfascial planes (Fig. 10.17.1.6).
Location: The retromesenteric plane is the fascial plane located between the anterior pararenal space and the perirenal space. The potential space between the layers of the lateroconal fascia is termed as the latero conal plane. The retrorenal plane separates the perirenal space from the posterior pararenal space, while the combined interfascial plane is formed by the inferior fusion of the retromesenteric and retrorenal planes which continues into the pelvis.
Communication and extent: The anterior interfascial retromesenteric plane is continuous across the midline, and communicates laterally with the lateroconal and retrorenal planes, at the fascial trifurcation. The combined interfascial plane extends into the pelvis, along the anterior to the psoas major and communicates with the extraperitoneal presacral and perivesical spaces. This communication can thus serve as a pathway of disease extension from the abdominal retroperitoneum into the pelvis and vice versa (Fig. 10.17.1.7).
In addition, the retrorenal plane communicates with the fascia transversalis via two pathways: (1) a cleft at the lumbar triangle, located between the medial border of the posterior pararenal space and the lateral border of the quadratus lumborum fat pad and (2) another narrow passage which connects the retrorenal plane with the subfascial plane, located between the posterior pararenal space anteriorly and the fascia transversalis posteriorly.
Applied anatomy: An understanding of the interfascial planes is crucial as various diseases involving the retroperitoneal organs can easily involve the interfascial planes and spread along them to involve other subsites. On CT or MRI, any fluid collection within these potential spaces tends to be sharply defined with linear or curvilinear margins. Thickening of the retroperitoneal fasciae on cross-sectional imaging is indicative of the presence of disease in the retroperitoneal organs and requires a detailed evaluation for the same. Several disease entities, both inflammatory and neoplastic can involve the interfascial planes, as follows:
• Acute pancreatitis: CT imaging is commonly used to assess the severity of pancreatitis by detecting the presence and extent of pancreatic necrosis and associated peri-, extrapancreatic fluid collections in the retroperitoneum, peritoneal cavity and rarely mediastinum. Often, inflammatory fluid collection initially accumulates in the anterior pararenal space, extends posteriorly to involve the anterior interfascial retromesenteric plane (Fig. 10.17.1.3). This collection may further spread posteriorly via the fascial trifurcation to the renorenal plane and extend to the flank via the subfascial plane between the posterior pararenal space and the transversalis fascia, giving rise to the flank discoloration in patients with pancreatitis, termed as the ‘Grey Turner’s sign’. Tracking of fluid into the subfascial plane can be identified by means of the ‘Checkmark sign’, which is an indicator of severe disease.
Haematomas resulting from great vessel injuries (Fig. 10.17.1.8): Haemorrhage resulting from rupture of aortic aneurysms or IVC injuries can extend to the retroperitoneum via the interfascial planes. Abdominal aortic aneurysms tend to bleed posteriorly and the resulting haemorrhage may extend into the left renorenal plane. Aortic haemorrhage may also track into the pelvis via the combined interfascial plane and present as a groin haematoma and rarely via the retromesenteric plane leading to compression of adjacent viscera such as the duodenum or colon resulting in features of intestinal obstruction. The IVC on the other hand, usually bleeds directly into the right renorenal plane, with haemorrhage also involving the perirenal spaces. Extension of haemorrhage into the subfascial plane, is depicted by the checkmark sign on imaging, which is associated with a worse prognosis and a higher mortality rate.
Perirenal haematomas: resulting from renal or adrenal injuries may extend into the retromesenteric and retrorenal planes by means of bridging septae which traverse the perirenal space. The haematoma may further extend into the pelvis via the combined interfascial plane (Fig. 10.17.1.9).
Urinomas: could occur secondary to forniceal rupture due to an obstructing renal calculus. CT imaging demonstrates encapsulated collections of urine in the perinephric space with leak of contrast material into the collection. The fluid which may in turn gain access to the retromesenteric plane via the bridging septae.
Duodenal perforation: resulting from blunt trauma or peptic ulcer disease could lead to leakage of fluid and air which may decompress into the retromesenteric plane. These can readily extend along the interfascial planes to distant sites (Fig. 10.17.1.10).
Spread of malignancies:
Involvement of the perinephric space could occur via its rich lymphatic network that drains the renal hilar lymph nodes, which in turn communicate with paraaortic and paracaval lymph nodes. Pleural and transdiaphragmatic lymphatics connect with the perinephric lymphatic network; which can potentially lead to metastases from a lung cancer into the perinephric space.
Infection and inflammation:
The ascending and descending mesocolon are in close proximity with the retromesenteric and lateroconal interfascial planes, thus infectious and inflammatory conditions of the ascending and descending colon, such as colitis, diverticulitis and retrocaecal appendicitis, can spread into the interfascial planes.
Fig. 10.17.1.6Schematic transverse section depicting the anatomy of the inter-fascial planes of the retroperitoneum, their communication and extent.
Fig. 10.17.1.7Schematic sagittal section depicting the anatomy of the interfascial planes of the retroperitoneum, their communication and extent.
Fig. 10.17.1.8Contrast-enhanced axial (A–D) and sagittal CT (E) sections in a case of a pelvic retroperitoneal haematoma. The right kidney appears bulky with perinephric fat stranding. Active leak of contrast from the right external iliac artery is seen on the arterial phase (blue arrow in A) with a resultant large haematoma (asterisks in A–D). Superiorly, it extends along the combined interfascial plane into the perirenal space (blue arrow in E) as well as along the retromesenteric (blue arrows in C and D) and retrorenal planes (asterisk in C). Medially the haematoma tracks into the central compartment (asterisk in D) via the perirenal space.
Fig. 10.17.1.9Contrast-enhanced axial (A, B) and sagittal CT (C) sections in a case of a perinephric haematoma (asterisks in A and B). It extends into the retromesenteric and retrorenal planes by means of bridging septae which traverse the perirenal space (blue arrow in A). Inferiorly, it extends along the combined interfascial plane into the pelvis (blue arrow in C).
Fig. 10.17.1.10Axial CT sections (A, B) in a case of duodenal perforation diagnosed following administration of oral positive contrast. The extravasated contrast extends into the retromesenteric plane (blue arrow in B).
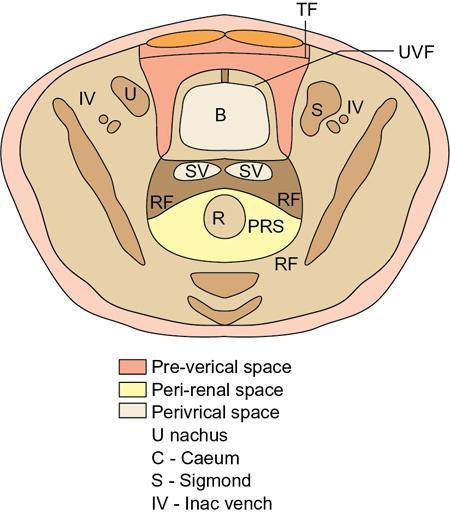
Pelvic extraperitoneal spaces
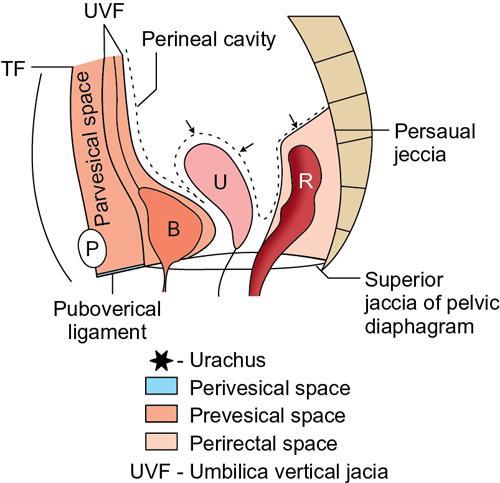
These are situated between the transversalis fascia and the parietal peritoneum, and include the prevesical, perivesical and perirectal spaces (Figs. 10.17.1.11 and 10.17.1.12). Anterior to the peritoneal cavity and posterior to the transversalis fascia, lies the umbilicovesical fascia (UVF). It has a triangular shape with its apex at the umbilicus, extending inferiorly to surround the urinary bladder, obliterated umbilical arteries and urachus. The UVF separates the prevesical space anteriorly from the perivesical space posteriorly.
The prevesical space: It is located anterior to the UVF and posterior to the transversalis fascia. It extends up to the umbilicus superiorly and inferiorly behind the pubis. Inferiorly, just posterior to the pubis, it is designated as the space of Retzius. The prevesical space is contiguous with the rectus sheath, the presacral space as well as the femoral sheath. Thus, rectus sheath haematomas as well as femoral sheath haematomas may extend into the prevesical space and cause compression of the pelvic viscera.
Prevesical space fluid/blood collections assume a ‘molar tooth’ configuration on axial CT and MRI images due to the presence of the UVF. The ‘crown’ of the tooth lies between the fascia transversalis and the UVF, displacing the bladder posteriorly; while the roots extend laterally between the UVF and the peritoneum.
The perivesical space: It is a thin space, enclosed by the UVF which contains the urinary bladder, urachus, obliterated umbilical arteries and fat. The perivesical space lies in contact with the prostate, seminal vesicles in males and the cervix in females. Fluid collections within the perivesical space are generally small and may be confused with bladder wall thickening on CT images. The perivesical space communicates with the prevesical and perirectal spaces.
Both, the prevesical as well as the perivesical spaces communicate with the abdominal retroperitoneum, which includes the perirenal space and the anterior/posterior pararenal spaces via the infrarenal compartment; thus accounting for pelvic extension of retroperitoneal collections.
The perirectal space: It contains the rectum, perirectal adipose tissue and the haemorrhoidal vessels. It is enclosed by the rectal fascia, which in its anterior aspect extends along the posterior surface of prostate and seminal vesicles in males and along the uterus and vaginal fornix in females. In its posterior aspect, the fascia lies parallel to the sacrum. Superiorly, it attaches to the peritoneal reflection. The perirectal space communicates with the prevesical and perivesical spaces.
Fig. 10.17.1.11Schematic sagittal section depicting the anatomy of the pelvic retroperitoneum and its fascial planes. The prevesical, perivesical and perirectal spaces are depicted. The umbilicovesical fascia separates the prevesical space anteriorly from the perivesical space posteriorly.
Fig. 10.17.1.12Schematic axial section depicting the anatomy of the pelvic retroperitoneum and its fascial planes. The prevesical, perivesical and perirectal spaces are depicted in the axial plane.
10.17.2
IMAGING TECHNIQUES AND PROTOCOLS FOR THE RETROPERITONEUM
Tanvi Vaidya, Shivani Mahajan
Introduction
Disorders of the retroperitoneum often have subtle, nonspecific and variable clinical signs and symptoms and hence their diagnosis is often challenging.
Cross-sectional imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MR) allow excellent, noninvasive evaluation of the normal anatomy and pathology and so are routinely preferred techniques for assessment of suspected retroperitoneal abnormalities.
Although retroperitoneal neoplasms have overlapping imaging features, a systematic image-based approach can help narrow the differential diagnosis.
Imaging techniques and protocol
Conventional radiography
Conventional radiographic means do not provide an accurate evaluation of retroperitoneum. The blurring of the psoas margins may be seen in mass lesions but is nonspecific. Intravenous urography may show secondary features such as ureteral obstruction and hydronephrosis. Transvertebral retroperitoneal gas insufflation is an obsolete historical radiographic technique that involved the injection of gas into the retroperitoneal spaces through the presacral route.
Ultrasonography
Evaluation of clinically suspected abdominal masses often begins with a transabdominal ultrasound examination. Often asymptomatic/clinically silent retroperitoneal lesions are incidentally detected on abdominal ultrasound. USG is an excellent tool for primary screening, for differentiation of solid from cystic lesions and also to guide interventions such as image-guided percutaneous biopsies or aspiration. But USG has certain drawbacks, such as poor definition of soft tissue planes, limited reproducibility and limited evaluation due to overlying bowel gas.
CT and MRI
Cross-sectional imaging techniques such as CT and magnetic resonance imaging (MRI) are the most widely used techniques in retroperitoneum imaging, and play a crucial role in accurate anatomic localization, disease characterization, evaluation of extent, adjacent organ invasion, distant organ involvement and staging. Both these techniques have multiple advantages such as short study time (5–10 minutes for a CT and 20–30 minutes for an MRI), high spatial resolution, multiplanar and volumetric display of data, the capacity of whole-body imaging, and good soft tissue contrast.
Computed tomography
CT is the primary and most widely used imaging modality in cases of clinically suspected retroperitoneal pathology and also for in-depth evaluation and characterization of ultrasonographically encountered retroperitoneal lesions. CT provides excellent anatomic details, has high spatial resolution, and aids in accurate compartmentalization of the disease. CT is superior to MRI in detecting calcifications, ossification and gas, and is often more accessible than MRI, and can be used when MRI is contraindicated.
The CT protocol depends on the type of scanner and the indication for the study. Careful attention should be paid to patient preparation and technical details of the scan. Five- millimetre thick slice with 1–2 mm detector collimation is routinely used for a survey examination on a 4–16 slice multidetector-row CT (MDCT). Thinner collimation of 0.5–0.7 mm is used for the angiographic examination of the abdominal aorta and its main branches on an MDCT. Multiplanar image reconstruction can be done at 1–2 mm intervals.
CT examination of the retroperitoneum is always performed after the ingestion of oral contrast medium, except in case of emergencies such as a suspected ruptured aortic aneurysm. The patient is asked to ingest approximately 1000 mL of oral contrast material (such as dilute barium suspension or iodinated water-soluble contrast material) about 1 hour before the examination to opacify the distal small bowel and large bowel, followed by 300–500 mL of contrast 15 minutes before the study to distend the stomach and proximal small bowel. In addition, 200 mL of contrast can be administered per rectally to opacify the rectum and sigmoid colon. CT examination is performed with the patient in a supine position with axial sections extending from lung bases to pubic symphyses. Precontrast images are acquired for detection of haemorrhage, calcification, ossification, macroscopic fat, cystic or necrotic changes and as a baseline scan to assess the degree of enhancement after IV contrast injection. Intravenous contrast is administered using a power injector at a rate of 2–3 mL/sec for regular survey examination and 3–5 mL/sec for CT angiography. CT angiography images are acquired 25 seconds after injection of contrast, followed by images in the venous phase at 60–70 seconds. Delayed-phase or excretory urography phase images at 5–10 minutes are useful for visualization of the pelvicalyceal system, ureters and bladder. The data set can be reconstructed in coronal, sagittal and oblique planes, and three-dimensional volume-rendered image can be created through postprocessing software.
Magnetic resonance imaging
MRI has certain advantages over CT such as lack of ionizing radiation, superior contrast resolution and can be used when CT contrast is contraindicated or contrast allergy is present. It is preferred over CT in pregnant and paediatric patients. Through the acquisition of various imaging sequences, MR allows a better understanding of the inherent characteristics of the disease pathology.
The MRI protocol for retroperitoneum is similar to that of abdominal imaging. MR examination is performed with a torso phased array coil using breathhold sequences. Both T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) aid in lesion detection and characterization. T1WI can be obtained using either SE (spin-echo sequence, TR 300–1000 msec, TE as short as possible) or GRE sequences (gradient echo sequences such as FLASH, GRASS etc.) GRE is preferred as multiple sections and can be acquired in a single breathhold and so high-quality images are obtained with no respiratory artefacts and minimal artefacts due to bowel peristalsis. Precontrast T1 GRE sequence is performed in both in phase and out of phase. T2WI (TR >1500 msec and TE >70 msec) can be conventional SE sequences or fast spin-echo (FSE)/turbo spin-echo (TSE) such as HASTE. The FSE has the advantage of significantly lesser image acquisition time and hence it is preferred. Diffusion-weighted imaging can be performed when necessary.
Standard MRI protocol of the retroperitoneum includes coronal SSFSE (single-shot fast spin echo) T2WI, axial FSE (fast spin echo) T2WI, axial T1WI with fat saturation, axial in-phase and out-of-phase T1WI and 3D T1-spoiled GRE breathhold sequence. Axial DWI may be acquired when necessary. Axial images are acquired with a 3-mm thickness and 2-mm interslice gap. Coronal and sagittal images help in better visualization of the aorta, IVC and the psoas.
High signal intensity fat/blood products, lymph nodes and vascular invasion are best seen on noncontrast TIWI. T2 fat-saturated images provide good visualization of lymph nodes, cystic changes, central tumoural necrosis, retroperitoneal fluid collections, marrow oedema and dilatation of ureters. Precontrast and postcontrast T1WI images (both arterial and venous phases) provide insights into the etiopathology of the abnormality. However, the delayed postcontrast T1WI is the most important sequence for characterizing the nature of the disease (solid or cystic), define the disease extent, detect vascular thrombosis, evaluate vascular encasement by the tumour and for screening the abdomen and pelvis.
Gadolinium-based intravenous contrast is routinely used in retroperitoneal imaging. The recommended dose is 0.1–0.2 mmol/kg of body weight given as a bolus injection at a rate of 2 mL/sec. FLASH images are acquired at 45 seconds followed by fat-saturated FLASH sequences at 90 seconds.
MR angiographic (MRA) images can be acquired using GRE sequences based on time of flight (TOF) of phase-contrast (PC) techniques. The 2D TOF requires less time and is accurate, but has the disadvantage of in-plane flow saturation in slow flow and tortuous vessels. The PC technique is more sensitive to flow but is time consuming and there is signal loss in turbulent flow. Three-dimensional gadolinium-enhanced GRE MRA overcomes the limitations of both these 2D angiography techniques and is based on the principle of T1 shortening by gadolinium contrast. The 3D images acquired can be reconstructed with maximum intensity projection (MIP) so that the entire arterial and venous system can be viewed in multiple projections. MRA requires a contrast dose of 0.1–0.2 mmol/kg of body weight at a rate of 2–3 mL/sec with a power injector, followed by 15 mL of normal saline.
Despite the many advantages of CT and MRI, they often fail to provide a definite diagnosis or differentiate between benign or malignant lesions. In such cases accurate percutaneous-guided biopsies can be performed under USG, CT or MR guidance to arrive at a conclusive diagnosis (Tables 10.17.2.1–10.17.2.2).
Axial GRE T1 Chemical shift imaging – in phase and out of phase
3D GRE volumetric interpolated fat-saturated breathhold sequence
Additional sequences – DWI, SWI
Noncontrast MR angiography – TOF/PC
Postcontrast
T1 fat saturated – Arterial, venous and delayed-phase images
Contrast MR angiography
Cross-sectional imaging-based approach to primary retroperitoneal neoplasms
Retroperitoneal tumours consist of a diverse group of pathologies, often with considerable overlap in imaging features. Radiological diagnosis of these lesions can be challenging and requires a stepwise image-based approach.
This consists of determining the precise tumour location (within the retroperitoneal anatomical space), identifying the most probable organ of origin, and detecting certain specific imaging features which further narrow down the differentials, such as the pattern of spread, degree of tumoural vascularity and the internal components (Fig. 10.17.2.1).
1. Tumour location:
A lesion located in the true retroperitoneal space will cause mass effect and resultant anterior displacement of normal retroperitoneal structures. This displacement of normal organs can be used to confirm the true retroperitoneal location of the pathology. Any lesion causing anterior displacement of the ascending or descending colon, duodenum, pancreas, adrenals or kidneys would suggest a lesion with primary retroperitoneal origin.
2. Organ of origin:
Once we have confirmed the primary location of the lesion, the next step is to determine the most probable organ of origin. Before labelling a tumour as a primary retroperitoneal neoplasm, it is imperative to rule out the possibility of it arising from a retroperitoneal organ. Radiological signs which aid in deciding the organ origin include: ‘organ-embedded sign’, ‘phantom organ/invisible organ sign’, ‘beak sign’, ‘feeding artery sign’.
Beak sign
If a mass deforms the margin of an adjacent organ into a beak shape, then the mass probably originates from that organ – this is the positive ‘beak sign’. On the contrary, if the mass has dull edges or fuzzy margins (no sharp beak seen) with adjacent organs, it indicates that the mass probably does not arise from the organ but just compresses it (Figs. 10.17.2.2–10.17.2.3).
Organ-embedded sign
If a part of the organ appears to be in close contact with the tumour or embedded in the tumour, the intervening contact surface may be sclerosed or occasionally ulcerated – this is the positive organ-embedded sign, the presence which indicates that the tumour originates from the involved organ (Figs. 10.17.2.4–10.17.2.5).
If a retroperitoneal tumour compresses an adjacent plastic organ which is not the organ of origin (such as compression of the intestine or IVC) then these plastic organs are deformed into a crescent shape – this is known as the negative embedded organ sign.
Phantom (invisible) organ sign
When a large mass originates from a relatively smaller organ, the primary organ of origin is often completely engulfed by the tumour and is not seen separately. This sign is seen in tumours of adrenal gland origin.
Prominent feeding artery sign:
Multiple prominent feeding arteries are seen on CT and MRI in the case of highly vascular tumours, and this aids in determining the origin of the tumour.
3. Patterns of spread
Extension between normal structures
Certain neoplasms tend to grow and spread in-between normal structures and encase vessels without causing luminal narrowing or compression. This is also known as a mantle growth pattern. Examples include lymphoma, lymphangiomas and ganglioneuromas. Lymphomas typically encase the aorta, IVC and major retroperitoneal vessels and displace the aorta anteriorly – this is known as the ‘floating aorta sign’ or the ‘CT angiogram sign’. Nonneoplastic diseases such as Erdheim–Chester disease and retroperitoneal fibrosis also present with mantle growth (Figs. 10.17.2.6–10.17.2.7).
Extension along with normal structures
Neoplasms of the sympathetic ganglia such as paragangliomas and ganglioneuromas appear elongated in shape and typically extend along the sympathetic chain.
4. Tumour components
Certain internal components of tumours detected through CT and MRI give important clues to narrow down the differential diagnosis significantly. These include fat, myxoid stroma, necrosis, cystic contents, small round cells, vascularity, calcifications and fibrosis.
Fat
A lipoma appears as a homogeneous tumour consisting entirely of fat. Fat shows low attenuation on CT with characteristic T1 hyperintensity with loss of signal on T1 fat-saturated MR images. Whereas an ill-defined irregular mass with fat content often represents a liposarcoma. High-grade liposarcoma may not contain appreciable amounts of fat and may appear similar to soft tissue sarcoma. Another common fat-containing retroperitoneal tumour is teratoma, which also contains fluid, fat fluid levels and calcification. Intralesional fat is also seen in extramedullary haematopoiesis, extraadrenal myelolipoma and cystic lymphangioma (Fig. 10.17.2.8).
Myxoid stroma
It consists of a mucoid matrix rich in acid mucopolysaccharides and appears T2 hyperintense with typical delayed contrast enhancement. Myxoid malignant fibrous histiocytomas, malignant liposarcoma and neurogenic tumours such as malignant peripheral nerve sheath tumour, ganglioneuroblastoma, ganglioneuromas, neurofibromas and schwannomas commonly contain myxoid stroma.
Necrosis
Often seen in high-grade malignant tumours such as leiomyosarcomas, undifferentiated pleomorphic sarcoma and pleomorphic liposarcoma. Necrosis appears as nonenhancing hypodense areas on CT and T2 hyperintense areas on MRI. Paragangliomas may contain central haemorrhagic necrosis and fluid–fluid levels due to their hypervascular nature.
Cystic contents
Lymphangiomas and mucinous cystic tumours are completely cystic, whereas neurogenic tumours such as schwannomas and neurofibromas are mixed solid cystic lesions. Schwannomas can be completely cystic and should be considered in the differentials of purely cystic masses. Myxoid liposarcoma, cystic mesothelioma, cystadenoma, cystadenocarcinoma, Müllerian cysts, epidermoid cysts and nonpancreatic pseudocysts are few of the other less common cystic lesions (Fig. 10.17.2.9).
Hyperattenuating cysts are usually posttraumatic haematomas or urinomas. Low-attenuation cysts with recent operative history of lymphadenectomy or renal transplant are lymphoceles.
Small round cells
Small round cell tumours such as lymphoma appear homogeneous on CT with minimal contrast enhancement and appear characteristically homogeneously hypointense on T2WI, due to densely packed cellular components.
Vascularity
Hypovascular tumours include low-grade liposarcoma, lymphomas and many benign tumours. Moderately vascular tumours are myxoid malignant fibrous histiocytomas, leiomyosarcomas and many other sarcomas. Tumours such as paragangliomas and haemangiopericytomas are extremely vascular and show intense contrast enhancement.
Progressive enhancement
Cystic masses with slow progressive enhancement include urinoma, due to gradual delayed contrast excretion into the urine, and lymphangioleiomyoma, due to slow lymphatic flow.
Calcifications
Solid retroperitoneal tumours with calcifications include dedifferentiated liposarcoma, neurogenic tumours, teratoma, extra gastrointestinal stromal tumour, undifferentiated pleomorphic sarcoma, malignant fibrous histiocytoma, chondrosarcoma, Ewing sarcoma and synovial sarcoma.
Fibrosis
Lesions with dense fibrosis appear hypointense on T2WI, such as desmoid tumour and nonneoplastic conditions such as retroperitoneal fibrosis and Erdheim–Chester disease.
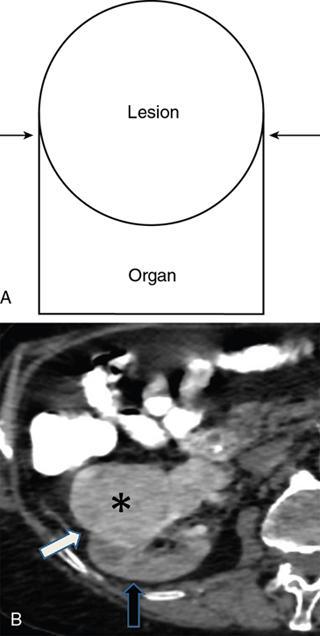
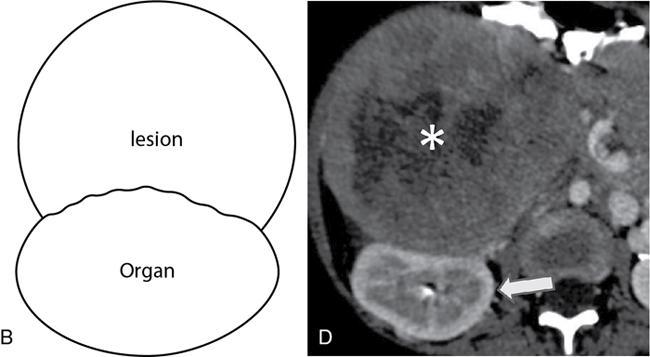
Fig. 10.17.2.1Positive beak sign – Drawing (A) shows beak-shaped interface (arrows) of lesion with organ. Axial CT (B) shows sharp beak like interface (white arrow) between the retroperitoneal enhancing mass (asterisk) and the kidney (black arrow) which implies the lesion arises from the organ.
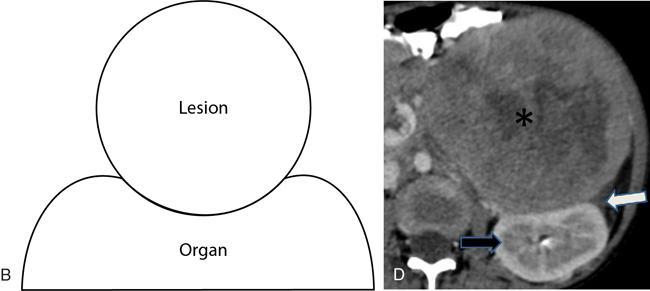
Fig. 10.17.2.2Negative beak sign – Drawing (B) shows dull rounded interface of lesion with organ. Axial CT (D) shows blunt interface (white arrow) between the retroperitoneal mass (asterisk) and the kidney (black arrow) which indicates the lesion does not arise from the organ. Source: Authors own
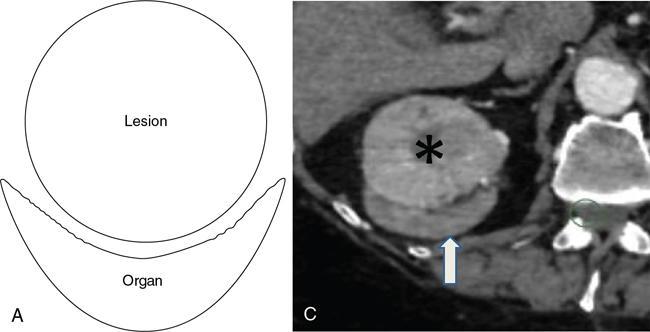
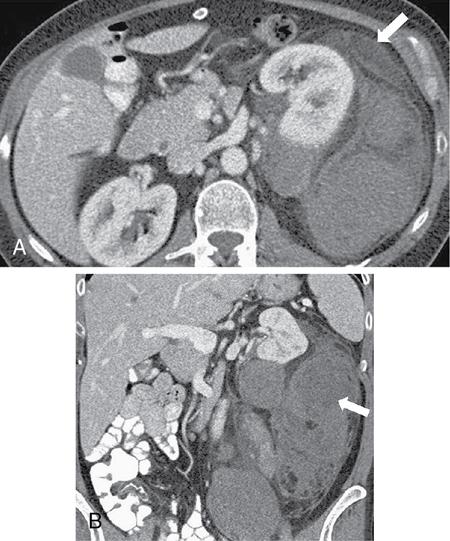
Fig. 10.17.2.3Negative organ-embedded sign – Drawing (A) shows lesion compressing the organ, and the organ becomes crescent shaped. Axial contrast-enhanced CT scan (C) shows adrenal lesion (asterisk) and crescent-shaped kidney (white arrow) with smooth interface between lesion and kidney. Source: Authors own
Fig. 10.17.2.4Positive organ-embedded sign – Drawing (B) shows lesion which appears to be embedded in organ at the contact surface. Axial CT (D) shows irregular contact surface between the renal mass (asterisk) and the kidney (white arrow). Source: Authors own
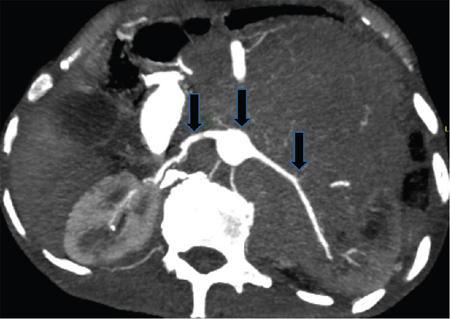
Fig. 10.17.2.5Mantle growth pattern – Axial CT angiogram in a 64-year-old male with DLBCL (diffuse large B cell lymphoma) shows the lymphomatous mass encases aorta and major retroperitoneal vessels (black arrows) by extending in between normal structures. Source: Authors own
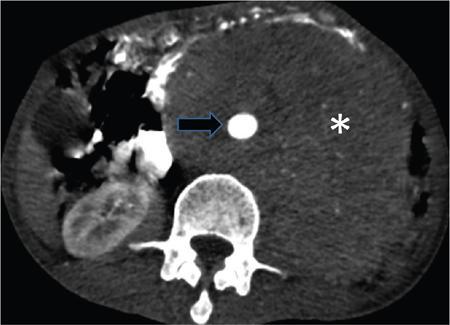
Fig. 10.17.2.6Axial CT scan (arterial phase) in a 70-year-old male with lymphoma shows the ‘floating aorta sign’ caused by anterior displacement of the aorta (black arrow) by the large hypodense retroperitoneal mass (asterisk). Source: Authors own
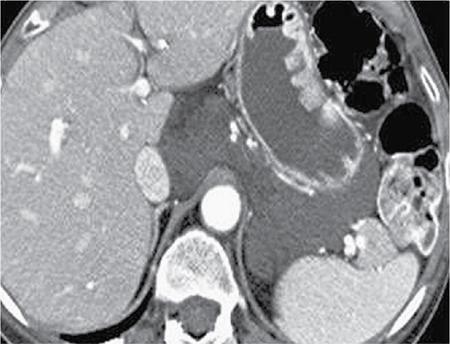
Fig. 10.17.2.7Well-differentiated liposarcoma. (Source: Courtesy of Ajit H. Goenka, Shetal N. Shah, Erick M. Remer. Imaging of the retroperitoneum. Radiol Clin N Am 50 (2012) 333–355. doi:10.1016/j.rcl.2012.02.004 0033-8389/12/$.)
Fig. 10.17.2.8Lymphangioma. (Source: Courtesy of Ajit H. Goenka, Shetal N. Shah, Erick M. Remer. Imaging of the retroperitoneum. Radiol Clin N Am 50 (2012) 333–355. doi:10.1016/j.rcl.2012.02.004 0033-8389/12/$.)
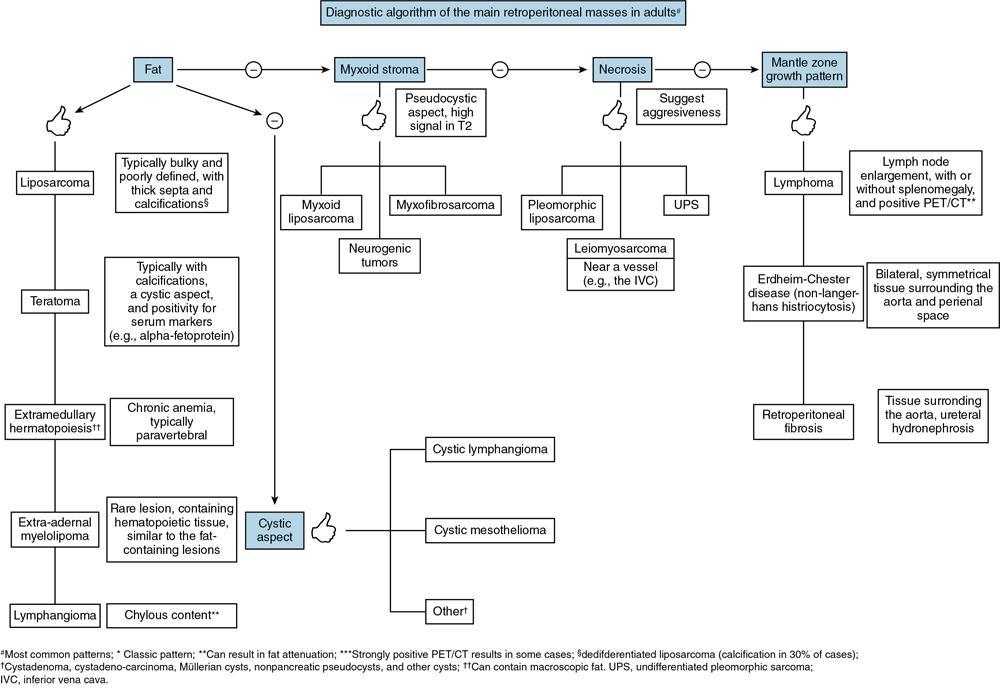
Fig. 10.17.2.9Diagnostic algorithm for evaluation of retroperitoneal masses. (Source: Courtesy of Mota MMS, Bezerra ROF, Garcia MRT. Practical approach to primary retroperitoneal masses in adults. Radiol Bras. 2018 Nov/Dez;51(6):391–400. Radiol Bras. 2018 Nov/Dez;51(6):391–400)
Conclusion
Lesions of the retroperitoneum include a diverse group of neoplastic and nonneoplastic diseases, including some rare conditions. Cross-sectional imaging techniques such as CT and MRI play an indispensable role in the detection and characterization of these lesions, and also in disease staging and hence are the modalities of choice for retroperitoneal imaging. A definite diagnosis may not always be possible based on cross-sectional images alone due to many similar and overlapping imaging features of these retroperitoneal tumours, but identifying specific characteristic imaging features along with clinical presentation helps to narrow the differential diagnosis.
10.17.3
SOLID NONNEOPLASTIC LESIONS
Tanvi Vaidya, Shivani Mahajan
Nonneoplastic conditions
Retroperitoneal fibrosis
Incidence
Retroperitoneal fibrosis (RPF) includes a range of diseases that are characterized by an excessive and aberrant proliferation of fibroinflammatory tissue, which surrounds the abdominal aorta, inferior vena cava and extends laterally to encase the ureters. RPF may be idiopathic (also known as Ormond’s disease) or secondary to malignancy, drugs such as methysergide, and bromocriptine and other aetiologies.
RPF is a rare disorder with an incidence of 1 per 200,000 populations. It commonly occurs in adults between the ages of 40 and 60 years and has a male predilection. There is no known familial or ethnic predisposition.
Aetiology
The precise aetiology of RPF is unclear but one of the proposed mechanisms is an immune reaction to a lipoprotein polymer called ceroid which is a component of ruptured atherosclerotic plaque. Another theory is the presence of an underlying systemic autoimmune process. RPF is associated with other fibrosing conditions such as fibrosing mediastinitis, sclerosing mesenteritis, orbital pseudotumour, primary sclerosing cholangitis and Riedel’s thyroiditis in up to 15% of cases. RPF is also associated with other autoimmune and inflammatory disorders such as systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis and asbestos exposure. Perianeurysmal fibrosis is seen in up to 25% cases of abdominal aortic aneurysm (known as inflammatory abdominal aortic aneurysm [IAAA]) and this is believed to be an early or mild form of RPF. A fibrotic desmoplastic response is initiated by metastatic foci to the retroperitoneum, commonly from lymphoma, retroperitoneal sarcoma, carcinoid tumours, carcinoma breast, lung, thyroid, stomach, colon, kidney, bladder, prostate and cervix, and this leads to malignant RPF. RPF can also occur secondary to infections (such as tuberculosis, syphilis, actinomycosis, fungi) or due to gastrointestinal inflammation (appendicitis, Crohn’s disease, diverticulitis). retroperitoneal haemorrhage or previous irradiation or surgery.
Histopathology
Gross pathological specimen examination reveals an ill-defined, greyish white, hard, plaque-like soft tissue mass usually at the level of the lumbar vertebrae, encasing the abdominal aorta, IVC, iliac vessels and the ureters. Rarely there is an anterior extension to the root of mesentery. Histologically the abnormal soft tissue is seen in two phases – early active inflammatory phase followed by the late chronic fibrotic phase. The process of maturation of the plaque progresses in a centrifugal manner from the midline so the central part is in the fibrotic phase and the lateral peripheral areas are inactive inflammatory phase. The early active cellular phase has immature periaortic fibrosis which is rich in perivascular inflammatory lymphocytes in a loose collagen matrix, and which is oedematous and high in vascularity. This is followed by the late inactive fibrotic phase where the collagen is gradually hyalinized and the cellularity decreases, to form the mature plaque which contains relatively avascular hyaline, is acellular, and contains scattered calcifications. Most of the inflammatory cells seen are positive for Ig G4 and HLA – DR on immunohistochemical analysis. RPF characteristically starts below the aortic bifurcation at the level of lower lumbar vertebrae, and progresses superiorly up to the kidneys in a periaortic and pericaval distribution, encasing one or both ureters. It may also extend inferiorly into the pelvis.
Clinical features
Signs and symptoms occur as a result of encasement and compression of retroperitoneal structures such as the aorta, IVC, ureters and gonadal vessels. Symptoms of idiopathic and secondary RPF often overlap and these are indistinguishable clinically. Initial symptoms are nonspecific with patients complaining of malaise, anorexia, weight loss, low-grade fever, vague abdominal pain or discomfort. As the soft tissue mass increases in size and extent, gradually specific symptoms are manifested according to organ involvement such as severe abdominal or flank pain, lower limb oedema, renal failure due to ureteric obstruction, testicular swelling in males and ovarian endometriosis in females. Almost 56%–100% of patients develop ureteric obstruction and eventual obstructive renal failure due to entrapment by the soft tissue. Renal vascular involvement may cause renovascular hypertension. IVC compression causes lower limb oedema and compression of aorta and its branches can cause lower limb claudication. Due to a lack of early specific clinical symptoms and often due to associated clinical disorders, the diagnosis is often delayed. Laboratory findings include altered renal function tests, elevated ESR and CRP.
Imaging features
Conventional abdominal radiographs are often unremarkable. Later stages may show a central abdominal soft tissue shadow with obscured normal psoas shadow, but these findings are variable. Complications of RPF may be seen such as dilated bowel in case of obstruction, pneumatosis in bowel infarction, nephrogenic pulmonary oedema, pulmonary fibrosis secondary to SLE, and ankylosing spondylitis, widening of mediastinum due to fibrosis. Features of Pott’s spine, ankylosing spondylitis and osseous metastases may also be seen.
Intravenous urography and retrograde pyelography have been obviated due to limited sensitivity and specificity and due to recent advances in cross-sectional imaging. The classic triad seen in IVU includes medial deviation of the middle third of the ureters, luminal tapering of ureters and a bilateral variable degree of hydroureteronephrosis with delayed contrast excretion.
The sensitivity of ultrasound in detecting RPF is low, and only 25% of cases detected on CT show a corresponding abnormality on USG. A well-defined irregularly marginated hypoechoic to anechoic plaque is seen in the prevertebral and paravertebral region, often with secondary hydroureteronephrosis. Abdominal ultrasound may aid in the diagnosis of associated conditions such as primary biliary cirrhosis, biliary strictures, portal hypertension, and sclerosing pancreatitis (Fig. 10.17.3.1).
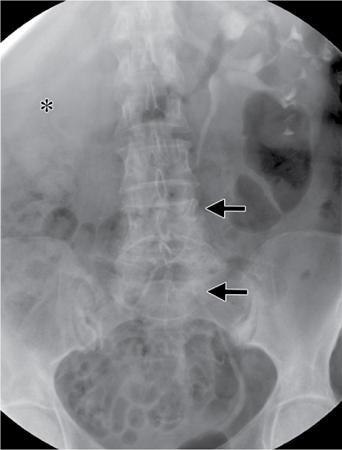
Fig. 10.17.3.1Urography of RPF. (Source: Courtesy of Rafael Oliveira Caiafa, Ana Sierra Vinuesa, Rafael Salvador Izquierdo, Blanca Paño Brufau, Juan Ramón Ayuso Colella, Carlos Nicolau Molina. Retroperitoneal fibrosis: Role of imaging in diagnosis and follow up. RadioGraphics 2013; 33:535–55.)
Only gold members can continue reading. Log In or Register to continue