Neoadjuvant chemotherapy is now widely used in the management of locally advanced breast cancer (LABC). Early initiation of systemic therapy can improve overall and disease-free survival for patients with LABC or inflammatory cancer. MR imaging with intravenous contrast and advanced MR imaging techniques provide new opportunities for assessing tumor morphologic changes, tumor vascularity, tumor cellularity, and tumor metabolic features. MR imaging is more reliable than the conventional methods in the assessment of tumor size and vascularity changes during and after chemotherapy. The addition of advanced imaging techniques to further characterize tumor cellularity and metabolic features appears promising. However, there is still no consensus on the role of MR imaging for assessing response to neoadjuvant chemotherapy or on a standardized MR imaging examination in patients receiving neoadjuvant chemotherapy.
Neoadjuvant chemotherapy (NAC) or primary systemic therapy given before surgery is now widely used as an alternative to the traditional approach of postoperative adjuvant chemotherapy in patients with breast cancer. Neoadjuvant chemotherapy is as effective as chemotherapy after surgery. Neoadjuvant chemotherapy is most often used in the treatment of patients with locally advanced breast cancer (LABC) because of the poor prognosis associated with this disease. The combination of NAC and surgery offers better local disease control and overall survival than surgery alone in patients with breast cancer, especially those with LABC. Moreover, NAC may allow the conversion of non-operable to operable disease or permit breast conservation therapy in patients who otherwise would have required mastectomy. However, a complete pathologic response to NAC does not occur in all patients. Therefore, it is important to identify early in the course of therapy which patients are likely to have a complete response to therapy and which patients are not. This information allows the physicians to tailor disease management and may improve patients’ outcomes and prolong survival.
It is imperative, therefore, that we identify the most accurate early predictor of response to therapy. Physical examination, mammography, and sonography (US) have all been used to assess response to NAC, but each of these approaches has limitations. Physical examination, though widely used for this indication, is unreliable and subjective, relying on the physician’s experience. Furthermore, physical examination cannot differentiate posttreatment fibrosis or residual necrotic tissue from residual viable tumor mass. Feldman and colleagues reported that 45% of complete clinical responders had macroscopic tumor at histologic examination, whereas 60% of patients without histologic gross residual tumor had an incomplete clinical response. In another series of 49 subjects, physical examination overestimated tumor regression in 23% of cases and underestimated response in 9%. Mammography may overestimate residual disease because of its inability to detect changes in the microcalcifications associated with the malignancy. Early series evaluating the role of US reported that US tends to underestimate residual tumor size and is actually less accurate than physical examination.
MR imaging is the first breast imaging modality that not only allows detailed visualization of the anatomy but also, when an intravenous contrast agent is administered or advanced sequences (eg, diffusion-weighted imaging or spectroscopy) are used, provides functional information. This article reviews the published data on the role of breast MR imaging in assessing tumor response in women receiving neoadjuvant chemotherapy.
MR imaging
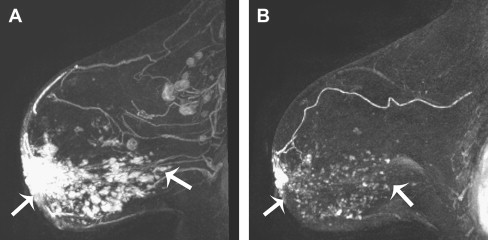
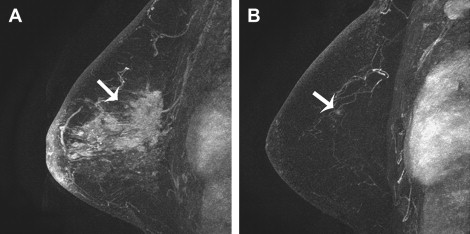
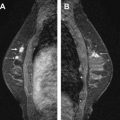
Breast MR imaging has a reported sensitivity of 95% to 97% for the detection of invasive breast cancer and 50% to 100% for the assessment of response to NAC ( Table 1 ). This high sensitivity is dependent on the ability of MR imaging to differentiate untreated hypervascular tumor from the background enhancing fibroglandular tissue or breast tissue. In patients undergoing neoadjuvant chemotherapy, the antiangiogenic effect of cytotoxic chemotherapy agents reduces the vascularity of the tumor mass. This decrease in tumor vascularity would be expected to be associated with a decrease in enhancement of that lesion on MR imaging ( Fig. 1 ). This dampening effect of chemotherapy on enhancement of the lesion may compromise the ability to visualize residual viable tumor. However, the alteration of tumor vascularity or other MR characteristics can help identify predictive features to differentiate patients whose cancer is likely to respond to the chemotherapy from those whose cancer would not respond ( Fig. 2 ). Since 1996, at least 37 studies have been published on the use of MR imaging in identifying such predictors. Many of these studies are single-institution trials with small sample sizes, ranging from 13 to 73 subjects. The studies vary in the criteria used for distinguishing complete responders from partial responders or non-responders. The MR imaging examinations performed in each trial are not standardized with regards to type of scanners, Tesla strength of the scanners, number and type of MR imaging sequences performed for each examination, number of post-contrast sequences performed, or timing of post-contrast sequences. Despite these differences, many of the observations from the studies were similar and are discussed in further detail later in this article.
| Authors | No. of pts | NAC | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|
| Abraham et al | 39 | B, A | 97 | — |
| Belli et al | 45 | B, D | 90 | 100 |
| Bhattacharyya et al | 32 | B, A | 88 | 50 |
| Choi et al | 41 | B, A | 71 | 95 |
| Warren et al | 67 | B, A | 100 | 80 |
MR imaging assessment of tumor size
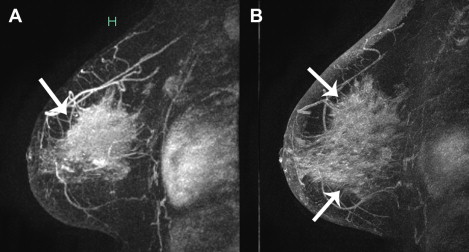
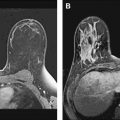
Accurate measurement of tumor size, before neoadjuvant chemotherapy, is important for staging, treatment monitoring, and determining prognosis. Tumor size has been known to predict patient survival and is the basis of most disease-staging systems. Studies have shown that imaging-based measurements are superior to clinical palpation in determining tumor size and predicting pathologic complete response. MR imaging more accurately reflects true pathologic tumor size and is more reliable than physical examination, mammography, or US in predicting the amount of residual disease after neoadjuvant chemotherapy ( Fig. 3 ). In one study, MR imaging measured the final tumor size accurately, to be within 1 cm of the final tumor size determined by gross histologic examination ( Fig. 4 ). In another trial of only 15 subjects, MR imaging overestimated main lesion diameter by only 3.4 mm, and this difference was not statistically significant. Several studies have shown that MR imaging prediction of tumor response to NAC correlates well with pathology, with the correlation coefficient (r) between MR imaging and histology ranging between 0.6 and 0.9. In one series, MR imaging correctly assessed the residual disease in 83% of the cases, with only one false negative case in which a 2 mm residual invasive carcinoma was not detected. MR imaging can underestimate residual disease in 2% to 10% of cases, especially if the tumor shrinkage pattern from the chemotherapy is patchy with areas of necrosis between nests of viable tumor or tiny tumor foci scattered over a large area. In a trial of 40 subjects with LABC, the underestimation was seen more frequently in patients treated with docetaxel-based chemotherapy than in those treated with 5-fluoro-uraci-epirubicin regimens. Overestimation of tumor size after neoadjuvant chemotherapy was reported in as many as 6% to 33% of the cases. These contradicting observations of underestimation and overestimation by MR imaging are derived from single institutional trials with small sample sizes; validation studies are needed with larger sample sizes and standardization chemotherapy regimens.
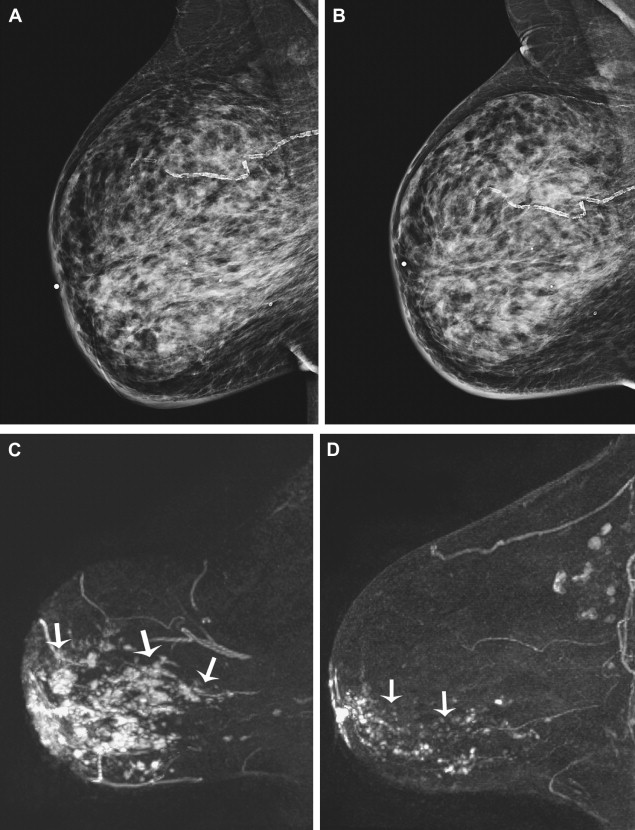
Some investigators have used tumor-volume calculations, in combination with largest tumor diameter to assess response to neoadjuvant chemotherapy. Some observed that a change in the initial and final tumor volume measurements by MR imaging had a stronger association with recurrence-free survival in those who received NAC compared with other prognostic indicators, such as largest tumor diameter. This volume change can be observed after only one cycle of chemotherapy and is suggested to be associated with recurrence-free survival. Other investigators compared the largest tumor size with tumor volume as possible predictors for response to therapy and noted that a tumor volume reduction of more than 65% after two cycles of chemotherapy was the most predictive value for predicting histologic response. Defining the margins of the breast tumors to accurately measure the largest diameter or calculate the tumor volume can be challenging during and after neoadjuvant chemotherapy. Additional information on tumor vascularity from contrast-enhanced MR imaging may be beneficial when combined with the morphologic assessment and size or volume change from NAC.
MR imaging assessment of tumor size
Accurate measurement of tumor size, before neoadjuvant chemotherapy, is important for staging, treatment monitoring, and determining prognosis. Tumor size has been known to predict patient survival and is the basis of most disease-staging systems. Studies have shown that imaging-based measurements are superior to clinical palpation in determining tumor size and predicting pathologic complete response. MR imaging more accurately reflects true pathologic tumor size and is more reliable than physical examination, mammography, or US in predicting the amount of residual disease after neoadjuvant chemotherapy ( Fig. 3 ). In one study, MR imaging measured the final tumor size accurately, to be within 1 cm of the final tumor size determined by gross histologic examination ( Fig. 4 ). In another trial of only 15 subjects, MR imaging overestimated main lesion diameter by only 3.4 mm, and this difference was not statistically significant. Several studies have shown that MR imaging prediction of tumor response to NAC correlates well with pathology, with the correlation coefficient (r) between MR imaging and histology ranging between 0.6 and 0.9. In one series, MR imaging correctly assessed the residual disease in 83% of the cases, with only one false negative case in which a 2 mm residual invasive carcinoma was not detected. MR imaging can underestimate residual disease in 2% to 10% of cases, especially if the tumor shrinkage pattern from the chemotherapy is patchy with areas of necrosis between nests of viable tumor or tiny tumor foci scattered over a large area. In a trial of 40 subjects with LABC, the underestimation was seen more frequently in patients treated with docetaxel-based chemotherapy than in those treated with 5-fluoro-uraci-epirubicin regimens. Overestimation of tumor size after neoadjuvant chemotherapy was reported in as many as 6% to 33% of the cases. These contradicting observations of underestimation and overestimation by MR imaging are derived from single institutional trials with small sample sizes; validation studies are needed with larger sample sizes and standardization chemotherapy regimens.
Related posts:
 Breast Magnetic Resonance Imaging: Current Clinical Indications
Breast Magnetic Resonance Imaging: Current Clinical Indications
 Implementing a Breast MR Imaging Program: All Things Considered
Implementing a Breast MR Imaging Program: All Things Considered
 Role of Magnetic Resonance Imaging in Evaluating the Extent of Disease
Role of Magnetic Resonance Imaging in Evaluating the Extent of Disease
 Probably Benign Lesions Detected on Breast MR Imaging
Probably Benign Lesions Detected on Breast MR Imaging
 A Clinical Oncologic Perspective on Breast Magnetic Resonance Imaging
A Clinical Oncologic Perspective on Breast Magnetic Resonance Imaging
 MR Intervention: Indications, Technique, Correlation and Histologic
MR Intervention: Indications, Technique, Correlation and Histologic
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


