and Clarisse Dromain2
(1)
Department of Radiology, San Giovanni Hospital, Roma, Italy
(2)
Department of Radiology, Institut de Cancerologie Gustav Roussy, VilleJuif – Paris, France
Abstract
The sandwich sign refers to the cross-sectional imaging appearance, most often on CT examination, of mesenteric fat and vessels as the sandwich filling, while the homogeneous soft tissue adenopathy represents sandwich bun. The sandwich sign is due to the presence of large bulky mesenteric adenopathy and is specific to mesenteric lymphomas. Mesenteric lymphomas are unique because they can grow to a large size and can envelop fat, bowel, and vessels without causing clinical symptoms. Most of these mesenteric lymphomas are NHLs. However in patients who have undergone transplantation, PTLD (posttransplant lymphoproliferative disorder), an Epstein–Barr virus-driven B-cell lymphoproliferation in immunosuppressed patients who have undergone transplantation can also create a sandwich sign.
Sandwich Sign
The sandwich sign refers to the cross-sectional imaging appearance, most often on CT examination, of mesenteric fat and vessels as the sandwich filling, while the homogeneous soft tissue adenopathy represents sandwich bun.
The sandwich sign is due to the presence of large bulky mesenteric adenopathy and is specific to mesenteric lymphomas. Mesenteric lymphomas are unique because they can grow to a large size and can envelop fat, bowel, and vessels without causing clinical symptoms. Most of these mesenteric lymphomas are NHLs. However in patients who have undergone transplantation, PTLD (posttransplant lymphoproliferative disorder), an Epstein–Barr virus-driven B-cell lymphoproliferation in immunosuppressed patients who have undergone transplantation can also create a sandwich sign.
Scleroderma, GI Tract
Scleroderma is a disease of unknown etiology characterized by widespread disorder of microvasculature and overproduction of collagen causing exuberant interstitial fibrosis with atrophy and sclerosis of many organs and systems; the skin is the most common affected tissue.
However important gastrointestinal manifestations of scleroderma are described: esophageal manifestation is quite common (hypotonia and aperistalsis and dysphagia), followed by stomach involvement (gastric dilatation, delayed empty), small bowel (malabsorption due to bacterial overgrowth and delayed transit time and jejunal dilatation with pseudosacculation due to smooth muscle atrophy) and colon (constipation with pseudosacculation, complete loss of haustration, and marked dilatation, bacterial overgrowth, and cystic pneumatosis).
In case of small bowel involvement, the duodenal and jejunal dilatation may simulate a small bowel obstruction leading to a misdiagnosis and unnecessary exploratory surgery.
Sigmoid Volvulus
Sigmoid volvulus usually affects elderly patients presenting with anatomical long sigmoid mesentery (Fig. 1). Sigmoid twist on mesenteric axis, the degree of torsion is variable (from 180° to 360° up to 540°). Twisted sigmoid colon appears as a greatly distended paralyzed loop (coffee bean sign at plain X-ray), with inverted U-shaped distended sigmoid colon and absence of air in the rectum detectable at CT scout view.
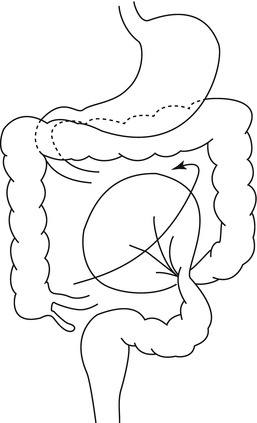
Fig. 1
Graphic illustrates the mechanism of sigmoid volvulus formation due to torsion and various degrees of rotation of the sigmoid colon with respect to the sigmoid mesentery
At CT the presence of distended sigmoid colon with two transition zones in the same point is the sign of a severe sigmoid twisting. Whirl sign with tightly torsioned mesentery formed by twisted afferent plus efferent loop is another sign of severe twisting.
Situs Viscerum Inversus
Situs viscerum inversus is a congenital malposition (complete or partial) of organs. It can be associated or not with Kartagener syndrome (autosomal recessive disease with defective cilia motility leading to situs viscerum inversus, chronic sinusitis, and bronchiectasia). Considering the bowel the malposition of the gastrointestinal tract is referred as partial or complete intestinal malrotation. Important anatomical landmark in case of intestinal malrotation is represented by positioning of the third portion of duodenum and Treitz ligament, positioning of jejunal loop, and the site of the cecum.
Small Bowel Benign Tumor
Benign tumor are quite rare in the small bowel. Leiomyoma is the most common benign tumor of small bowel. This is a benign smooth muscle tumor that arises in approximately 50 % of cases in the jejunum, followed by the ileum. Almost one half of all lesions are less than 5 cm. Other types of benign small bowel tumor are lipomas, angiomas, adenomas, neurofibromas, and fibromas.
In 50 % of cases the tumor is asymptomatic. Otherwise, the common clinical presentation is a history of bleeding from the bowel, anemia, and obstruction. Bleeding is less frequent in case of lipomas which are predominantly developed in the ileum with a high incidence of intussusceptions.
CT enteroclysis which combines the advantages of CT (extraluminal information) and conventional enteroclysis (distension of small bowel and lumen content analysis) is the imaging modality of choice for the detection of small bowel tumors. However it has a variable value. Indeed, intramural lesions that were totally in the wall of the bowel could be missed. Submucosal tumor produces filling defect, whereas subserosal tumor grows larger and has most often an exophytic component. Leiomyomas have a median size of 5 cm at time of diagnosis, round shape, sharp margins, and homogeneous density. Calcifications are occasionally detected. Intestinal lipomas are well-circumscribed masses of fat tissue with low CT density arising within the submucosa and occasionally surrounded by a capsule.
Video capsule endoscopy (VCE) and double-balloon endoscopy (DBE) have recently been introduced in clinical practice, to evaluate obscure bleeding in the small intestine. VCE is intended mainly to screen patients because it is not invasive. On the other hand, DBE is often the first diagnostic modality when a small bowel lesion is strongly suggested. Moreover DBE allows to perform biopsies and to determine the most appropriate surgical approach.
Small Bowel Malignant Tumor
Malignant neoplasms of the small bowel are among the rarest types of cancer, accounting for only 2 % of all GI cancers. Adenocarcinoma, lymphoma (see lymphoma), and carcinoid tumors (see carcinoid) account for the majority of small intestine malignancies. Adenocarcinoma is the most common histological type. Its prevalence tends to increase with age, with a mean age at diagnosis of approximately 60 years. Similar to adenocarcinomas in the colon, those in the small bowel arise from premalignant adenomas occurring both sporadically and in the context of familial adenomatous polyposis. Approximately 50 % arise in the duodenum, 30 % in the jejunum, and 20 % in the ileum. Leiomyosarcoma is an extremely rare malignant mesenchymal tumor of smooth muscle and accounts for between 5 and 10 % of soft tissue sarcomas. They should be differentiated from gastrointestinal stromal tumors (GISTs) that are often CD34 immunoreactive and express tyrosine kinase c-kit (CD117) receptor activity, in contrast to leiomyosarcomas.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


