and Sofia Gourtsoyianni2
(1)
UOC Radiologia BR, Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy
(2)
Imaging 2, Level 1, Lambeth Wing St Thomas’ Hospital, London, UK
Secretin MRCP
Secretin is an endogenous hormone normally produced by the duodenum and secreted in response to increased intraluminal acidity, which stimulates the exocrine secretion of the pancreas.
Synthetic human secretin can be administered during MRCP at the dose of 1 ml/10 kg of body weight or 0.2 μg/kg of body weight to induce secretion of bicarbonate-rich fluid from pancreatic ductal cells and a transient increase in the tone of the sphincter of Oddi, resulting in improved visualisation of the pancreatic ductal system.
After intravenous injection, the authors scan patients with a coronal single-shot turbo SE sequence, repeated every 30 s for 10 min. After this interval, a respiratory synchronised 3D turbo SE sequence can be acquired.
The effect of secretin starts immediately and peaks 3–5 min after the injection, when the calibre of the main pancreatic duct is increased by 1 mm or more compared to baseline. After 10 min the calibre of the main pancreatic duct should return to baseline; a persistent dilatation of >3 mm is considered abnormal.
Common indications for the use of secretin MRCP include the detection and characterisation of pancreatic ductal anomalies and strictures, characterisation of any communication between the pancreatic duct and cystic lesions, evaluation of the integrity of the pancreatic duct and assessment of pancreatic function and sphincter of Oddi dysfunction.
Serous Cystic Adenoma
Serous cystic adenoma (SCA) is a cystic tumour composed of cysts of different size, containing a fluid with glycogen and various degrees of proteins but no mucin. Based on their morphology, they are classified as having a polycystic (70 % of cases), honeycomb (20 %) or oligocystic pattern (<10 %). SCAs are usually asymptomatic until they become large enough to cause duodenal or common bile duct obstruction; only in these cases surgery should be suggested. At MR imaging, a macrocystic pattern and a size >3 cm at the time of diagnoses can be predictive of lesion enlargement.
Microcystic Serous Cystadenoma
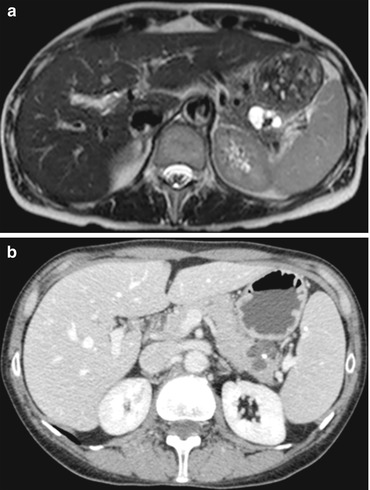
Serous microcystic cystadenoma is a benign pancreatic tumour occurring most commonly in females over 70 years (“the grandmother lesion”). The most common location is the pancreatic head or neck, but they have been described in all locations. SCA is usually an incidental finding at imaging, although larger lesions can cause nausea or abdominal pain. Microcystic serous cystadenoma is composed of multiple small cysts (usually >6) of varying sizes but always less than 2 cm of diameter with the larger cysts located peripherally, separated by thin septa. SCA typically has lobulated margins and does not have a capsule. Punctate or coarse calcifications can be present in more or less 20 % of the cases, usually in lesions larger than 5 cm. At MR imaging these lesions have a typical appearance; therefore further investigations and fine-needle aspiration are usually not required.
CT typically demonstrates a multicystic, lobulated mass in the pancreatic head region. A characteristic enhancing central scar may be present, which can show associated stellate calcifications.
At MRI, the cyst content is hyperintense on T2-weighted images and usually hypointense on T1-weighted images. Sometimes hyperintense areas on T1-WI can be present, due to previous intracystic haemorrhage. Fibrotic components are hypointense on T1-WI. Calcifications are hypointense both on T1- and T2-weighted images. The multiple thin septa radiating from the central scar show strong enhancement after gadolinium administration resulting in the so-called honeycomb-like pattern, with persistent enhancement of the central scar on more delayed scans (Fig. 1). The arteries supplying the tumour are frequently enlarged. On DWI SCAs do not show a significant restriction in diffusion.