Fig. 2.1
Retrospective ECG-gated scan. The x-ray beam (in blue) is on through the entire cardiac cycle
Prospective Scanning
The vast majority of scanning can and should be done using the prospective ECG-triggered scanning technique, even in children and infants with very fast heart rates. This technique uses a nonspiral step-and-shoot axial scanning process in which the x-ray beam is on for a short time and is turned off as the table moves. The imaging window is approximately 50 % of the cardiac cycle. Because an infant’s heart rate is relatively high, short acquisition times with padding may be used to capture up to 50 % of the cardiac cycle to evaluate function (Fig. 2.2); when functional analysis is needed, 175 ms of padding should be used. The padding turns the tube on before the required acquisition time and leaves it on afterward, increasing the time the current is on to include more of the cardiac cycle (Fig. 2.3) for functional imaging. For prospective scanning, our tube current–body weight adjustment has three weight based settings. Typically, end systole is the time for imaging the coronary arteries in adults, with optimal visualization between 65 and 80 % of the cardiac cycle. In infants, the optimal time for imaging the coronary arteries typically is during systole, at 45–55 % of the cardiac cycle.
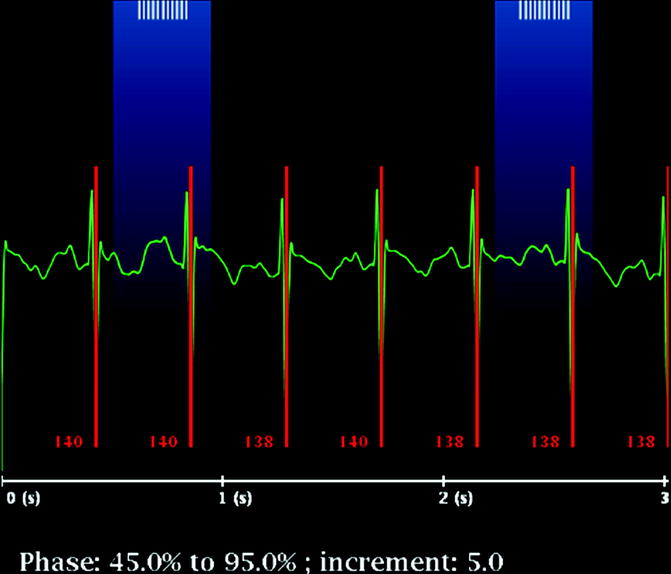
Fig. 2.2
Prospective ECG-gated scan. The x-ray beam (in blue) is not on during the entire cardiac cycle. Notice the rapid heart rate of 140 bpm. The rapid heart rate is advantage as the scan time covers enough of the cardiac cycle so that functional information can be obtained with provided with postprocessing
Fig. 2.3
Padding. Padding of 175 ms (yellow) is used to flank the acquisition time (green) to include more cardiac phases
Prospective Versus Retrospective Scanning (Table 2.1)
Table 2.1
Retrospective versus prospective ECG-gated scanning
Retrospective | Prospective |
|---|---|
Scans the entire cardiac cycle | Scans a variable portion of the cardiac cycle based on the padding time |
X-ray beam is on the entire time | X-ray beam is not on the entire time |
No padding is used | Padding may be used to cover parts of the cardiac cycle to obtain functional information |
Higher radiation dose | Lower radiation dose |
Radiation Dose
Children are more sensitive than adults to the effects of ionizing radiation; therefore, it is essential to balance image quality with radiation dose delivered when performing CTA in children. It is important to apply the ALARA (As Low As Reasonably Achievable) principle for infants and neonates by using low peak kilovoltage and adapting the milliamperes to the patient’s weight. Published studies comparing retrospective with prospective ECG-gated scanning techniques have reported radiation dose savings ranging from two to four times with prospective ECG-gated techniques [1–4]. Radiation doses estimated for prospective ECG-gated protocols have been reported to be less than 1 mSv in studies using low peak kilovoltage and low milliamperes per kilogram. On the contrary, retrospective ECG-gated scanning yields higher radiation doses, estimated to be around 3–10 mSv, even with the low-dose technique [5–10]. Another technique that may be used to lower the radiation dose for the patient is adaptive statistical iterative reconstruction, a unique CT reconstruction algorithm with matrix algebra used to selectively identify and subtract noise from the image. The result is less noise or the same amount of noise with less radiation [8–11].
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


