Kingston Vijay, Jansi Vinod, Sivakumar FOURNIER GANGRENE (NECROTIZING FASCIITIS): AN INFREQUENT TISSUE EATING DISEASE Fournier’s gangrene (FG): An awful infection of the visible genital region that causes grievous pain in the perineal area, which progresses from erythema to necrosis of tissue. FG is an acute dreadful urologic emergency, which has a high mortality rate of 15%–50%. It is a swiftly advancing, polymicrobial necrotizing fasciitis of the perineal, perianal and genital regions, which leads to reduced local blood supply causing vascular thrombosis in the skin and subcutaneous tissues. Subsequent spread of bacterial infection ensues with transfascial spread leading to development of gangrene of the overlying tissues. Fascial necrosis occurs at a rate of 2–3 cm/hr, making early diagnosis pivotal. Early diagnosis is essential and warrants surgical debridement and antagonistic triple antibiotic therapy. Computed tomography (CT) helps to confirm the diagnosis in clinically doubtful cases. In addition, radiography or ultrasound (US) can denote certain useful findings of FG, but CT has greater specificity for the diagnosis and displays the disease extent. Every radiologist must fathom out the imaging features of FG to document accurate diagnosis and urgent surgical treatment. FG is an acute terrible necrotic infection of the scrotum, penis and perineum. It is manifested as scrotal pain and redness with expeditious progression to gangrene and sloughing of tissue. FG is habitually secondary to perirectal or periurethral infections associated with local trauma, lower urinary infection and other operative procedures. The primary focus is located in the genitourinary tract, lower gastrointestinal tract and in the skin. FG is caused by both aerobic and anaerobic bacteria. It can eventually lead to multiple organ dysfunction syndrome (MODS) and death in severe cases. Owing to the dreadful complications, it is crucial to diagnose FG as quickly as possible. In spite of the antibiotics and surgical debridement, the death rate of FG remains high. It was first reported by Jean Alfred Fournier, who was a French professor of dermatology at St. Louis venereal hospital, the University of Paris in 1883. He observed a necrotizing gangrenous infection of male genitalia in young healthy males without any apparent source. The perineum is the area referring to the shallow internal compartment and external surface of the body (Fig. 11.11.1.1). The compartmental area of perineum is seen inferior to the pelvic outlet and is divided from the main pelvic cavity by the pelvic diaphragm. This pelvic diaphragm holds up the urogenital and gastrointestinal systems and plays an important role in defecation, micturition, sexual intercourse and labour. When viewed in subject with abducted thighs, the perineum resembles a diamond-shaped area that is bounded by the mons pubis anteriorly, medial aspect of the thighs laterally and the gluteal folds and upper end of natal cleft posteriorly and following osseofibrous boundaries: An imaginary transverse line connecting the anterior ends of the ischial tuberosities splits the perineum into two triangles: It is located in the rear half of the perineum. The sacrotuberous ligaments, the coccyx and an imaginary line connecting bilateral ischial tuberosities bound it. The major contents are: The main nerve of the perineum, the pudendal nerve is located in the anal triangle. The urogenital triangle is the front half of the perineum. It is bounded by pubic symphysis, ischiopubic rami, and an imaginary line between the two ischial tuberosities. Urogenital triangle has number of fascial layers and pouches and complex. Dissimilar to the anal triangle, the urogenital triangle has an extra layer of strong deep fascia, which is called as perineal membrane. The membrane has pouches on the superior as well as inferior surfaces (Fig. 11.11.1.3). The layers of the triangle (deep to superficial) (Fig. 11.11.1.4): Is located on the midpoint of theoretical transverse line joining the ischial tuberosities that is providing attachment to the perineal muscles. Perineal body lies deep to skin and subcutaneous tissue in the midline at the junction of anal and urogenital triangles. It is seen behind the vestibule of the vagina or bulb of the penis. Anus and anal canal are seen behind the perineal body. The perineal body is varying in size with little fat deep to the overlying skin (Fig. 11.11.1.6). All the perineal muscles converge in the perineal body and have three stratum. Superficial stratum includes bulbospongiosus, superficial transverse perenei muscles and superficial part of external anal sphincter. Intermediate stratum includes sphincter urethrae and deep transverse perenei muscle and deep part of the external anal sphincter. Deep stratum contains levator ani muscle. It is a triangle-shaped musculofascial diaphragm situated in anterior half of the perineum located in the region of the urogenital triangle filling space of pubic arch. It is pierced by urethra in both male and female and vagina in females. It holds the prostate gland and it constricts the vagina. It has: Infection of superficial perineal fascia (Colles’ fascia) may spread to the penis and scrotum across the Buck and Dartos’ fascia. Infection can spread into the anterior abdominal wall along the Scarpa’s fascia. Colles’ fascia limits progression of disease as it is attached to the perineal body and urogenital diaphragm posteriorly and to pubic rami laterally. Testis is rarely involved, as the testicular arteries originate directly from aorta. Well-advanced FG can extend from the fascial envelop of the genitalia throughout the perineum, across the torso and upper thighs. The superficial perineal space receives its blood supply from the internal pudendal artery, which is the branch of the internal iliac artery. Pudendal nerve and its branches are supplying the superficial perineal space. The posterior labial nerve, which is a branch of pudendal nerve has a medial and lateral branch and runs along the lateral part of the urethral triangle to supply the skin of the labia majora. The posterior scrotal nerve, which is branch of pudendal nerve has a medial and lateral branch and runs along the lateral part of the urethral triangle to innervate the skin of the scrotum. FG usually not only involves the corpora, urethra, testes, cord structures and deep muscular structures, but also the superficial and deep fascia as well as the skin. The infection spreads along the anatomical fascial planes. So knowing the routes of spread, familiarity with the perineal anatomy and its fascial planes is very important in understanding the potential pathways of disease spread. Thus if the Colles’ fascia is interrupted, then the infection can easily spread to the ischiorectal fossa and subsequently to buttocks and thighs. Urethral stricture Scrotal abscess Epididymo-orchitis Hydrocele Surgery/Aspiration Traumatic catheterization Urethral calculi Prostatic biopsy Vasectomy Perianal abscess Rectal biopsy Anal dilatation Haemorrhoidectomy Rectosigmoid malignancy Appendicitis Diverticulitis Strangulated inguinal hernia Infected Bartholin’s gland Vulval abscess Septic abortion Episiotomy wound Coital injury Genital mutilation In FG, rotting bacterial infection can cause microthrombosis of small subcutaneous vessels bringing about gangrene of the overlying skin. Cultures of FG wound often show poly microbial infections by aerobes and anaerobes, which include: Nonuniformity in clinical presentation. From subtle onset and slow progression to swift onset and fulminant course. Symptoms of FG include scrotal oedema, hyperemia, fever, pain, pruritus and crepitus. Crepitus is a common feature because of the presence of gas under the skin. Air in the soft tissues is produced by anaerobic bacteria and consists primarily of nitrogen, hydrogen, nitrous oxide and hydrogen sulphide. FG infection starts as cellulitis then necrotic patches start appearing over the skin and progress to extensive necrosis. Leucocytosis, anaemia, thrombocytopenia, dehydration, tachycardia, hypocalcaemia, and hyperglycaemia are the systemic manifestations of FG. FG can rapidly progress to septicaemia and multiple organ failure. Involvement of the testis is very rare, which suggests retroperitoneal origin or spread of infection. The diagnosis of FG is usually clinical. Imaging has an ancillary role. Radiologic evaluation is indicated when the diagnosis is not clearly established. The goals of radiologic evaluation are: Radiolucent soft tissue gas shadow may be seen over the scrotal or perineal region. The subcutaneous air pockets can enter from scrotum and perineum to the anterior abdominal wall, inguinal regions and thighs. Soft tissue air pocket visualized on X-ray of diabetic patients with FG in 100% of the cases, while physical examination can pick up scrotal wall air pockets only in 29% of the cases. High-resolution linear transducer (5–15 MHz) imaging of scrotum is a helpful tool in the diagnosis of FG prior to the clinical suspicious or physical examination of the disease. Ultrasound scan can show widespread abnormalities of scrotum such as scrotal wall oedema/cellulitis, testicular torsion, acute epididymo-orchitis, testicular trauma, necrotizing fasciitis and an obstructed inguinoscrotal hernia. Ultrasound can also display a thickened oedematous scrotal wall, air shadows within the scrotal wall, paratesticular fluid collection. Presence of subcutaneous air pockets in the scrotal wall with unhealthy echogenic white after shadows is the sonographic hallmark of FG. This distinct sonographic appearance of scrotal wall air shadows is due to fluid–air interface. Often the testis and epididymis are normal in size and echotexture because of different blood supply directly from abdominal aorta through testicular arteries. An obstructed inguinoscrotal hernia may show the presence of air shadows within the bowel loops or within the scrotal sac but not in scrotal wall layers. Many times ultrasound scan depicts the presence of air pockets in nearby subcutaneous soft tissues other than scrotal wall before physical examination does. Distribution of soft tissue air pocket may indicate the extent of the disease in multiple fascial planes. Scrotal wall emphysema may extend into the perineum, inguinal region and abdominal wall and occasionally into the thigh. Absence of scrotal wall emphysema dose not excludes the diagnosis of FG. CT is a very valuable tool in diagnosing and determining the extent of FG. Clear knowledge of the anatomy of perineal region and fascial planes, the extent of the disease can be established to a degree more specific than is possible with physical examination/sonography. CT is the modality of choice in FG. CT findings include: CT scan dominates in the detection of deep-seated perineal, pelvic and intraabdominal fluid collections, which is very important in the eradication of the disease. It also provides wide field of view of perineum, pelvis and proximal portion of the lower extremities. Retroperitoneal extension is also well demonstrated with CT. Extent into anal triangle and urogenital triangle can be clearly made out. CT screening of perineum and pelvis can frequently show the underlying cause of the FG such as urethral pathology, perianal abscess, fistulous tracts, incarcerated hernia and source of infection that may be from intraabdominal or deep pelvic process and helping to planning of surgical debridement and management. Posttreatment follow-up CT scan is very important in assessing for improvement or worsening of FG. CT is useful in deciding additional therapy or surgical excision. MRI scan of the pelvis and perineal region is used to assess the extent of FG along the tissue planes. MRI yields better soft tissue details than the CT scan (Fig. 11.11.1.8). STIR imaging displays the oedema/inflammation of skin, subcutaneous fat and inter muscular planes as hyperintense shadows. Air loculi present in interstices of scrotal wall appear as hypointensities. MRI scan clearly demonstrates the extension of FG inflammatory process into the inguinal canal, pelvic cavity and in ischiorectal fossa as bright hyperintense shadows. Prolonged time for MRI scan, patient monitoring difficulties, clinically unstable patients limit the practical usefulness of MRI scan. The mortality in FG is little high ranging from 3% to 45%. Factors associated with high mortality include: Early presentation in good functional status along with appropriate and timely treatment leads to a good outcome. FG wound extending more than 5% of the body surface area carries a poor prognosis. Abdominal wall or lower limb involvement has notable increase in mortality rate. Used for prognostication and predicting mortality probability in FG. This is a numerical score derived from a combination of nine physiological variables including temperature, respiratory rate, heart rate, creatinine, sodium, potassium, bicarbonate, white cell count and haematocrit. FGSI score more than 9 indicates 75% mortality probability while less than 9 indicates a 78% survival probability. FG is an infrequent but quickly growing disease that mostly affects men with certain comorbid risk factors. In spite of all advances in medical care, it still continuous to be a disease with high mortality. The early debridement of necrotic tissue is the paramount factor for survival. ABDOMINAL WALL HERNIA Hernia refers to the protrusion of a part or structure through the tissues normally containing it through either through stretching or opening in normal tissues. Hernia may be external/internal. Hernias are the frequent imaging findings in abdomen. Most are asymptomatic but chances of developing complications present like incarceration, strangulation and trauma are present, so often they are surgically repaired. Using linear 10 MHz transducer inguinal region is examined. In obese patients 7 MHz may be required. During Valsalva, manoeuvres characteristic movement of herniating tissues through the defect clinches the diagnosis. This dynamic imaging is the added advantage in ultrasound. If bowel is the content peristalsis noted. If fat is the content in the sac, it appears hyperechoic. BOX 11.11.2.1 CLASSIFICATION OF EXTERNAL HERNIA
11.11: Scrotum
Introduction
Definition
History and etymology
Epidemiology
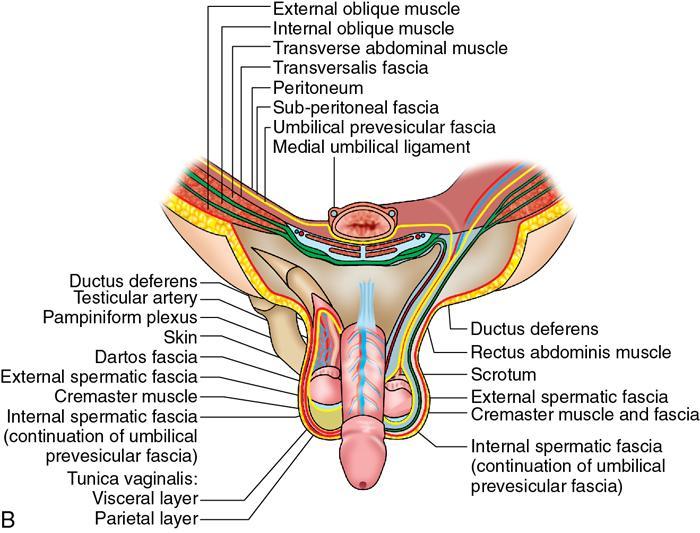
Relevant anatomy
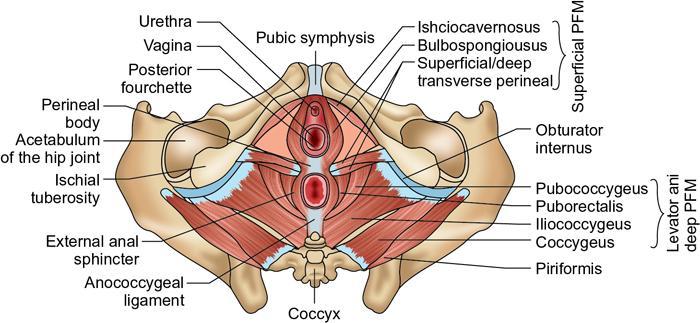
Perineum
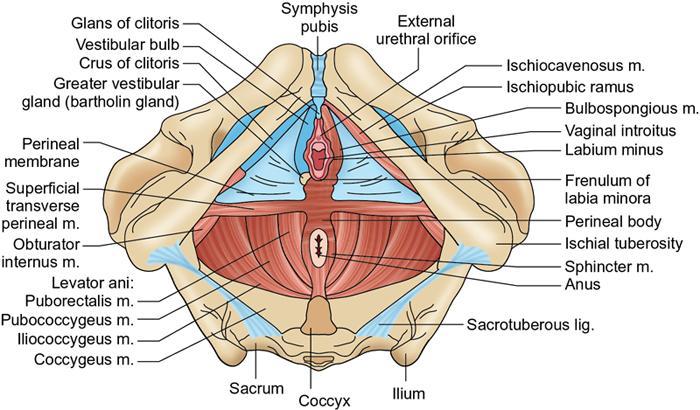
Extent and boundaries of perineum
Division of perineum (Fig. 11.11.1.2)
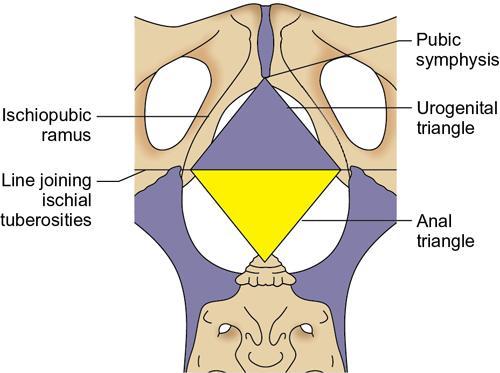
Anal triangle
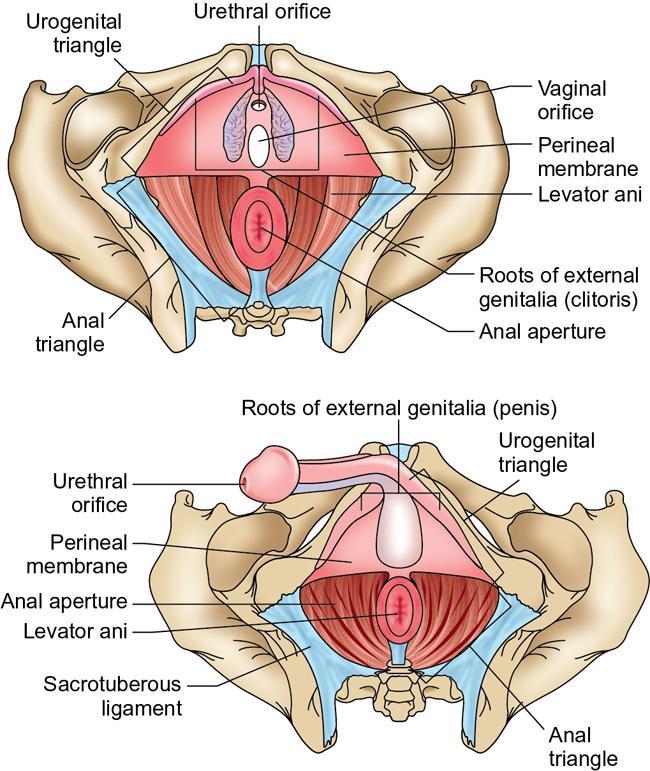
Urogenital triangle
Perineal body
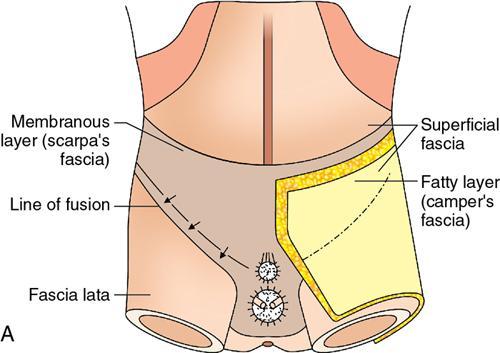
Perineal membrane and urogenital diaphragm
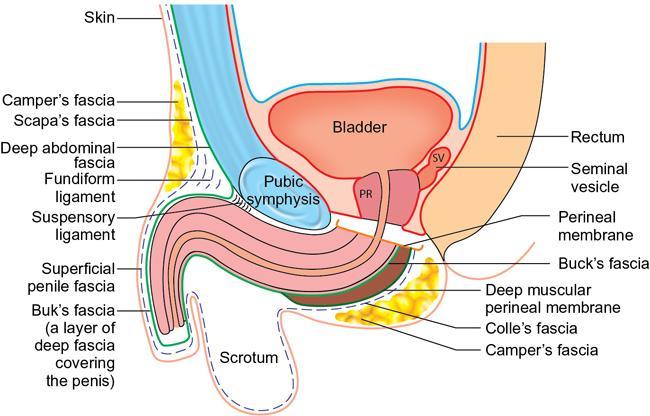
What is the significance of superficial perineal fascia (colles’ fascia) in the evolution of fournier gangrene?
Blood supply and lymphatics
Nerves
Aetiology
Urogenital
Anorectal
Gynaecological
Pathogenesis
Comorbid risk factors for FG
Clinical presentation
Differential diagnosis
Investigations
Radiologic features
Plain X-ray
Ultrasound
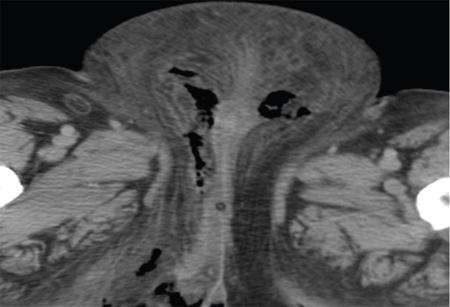
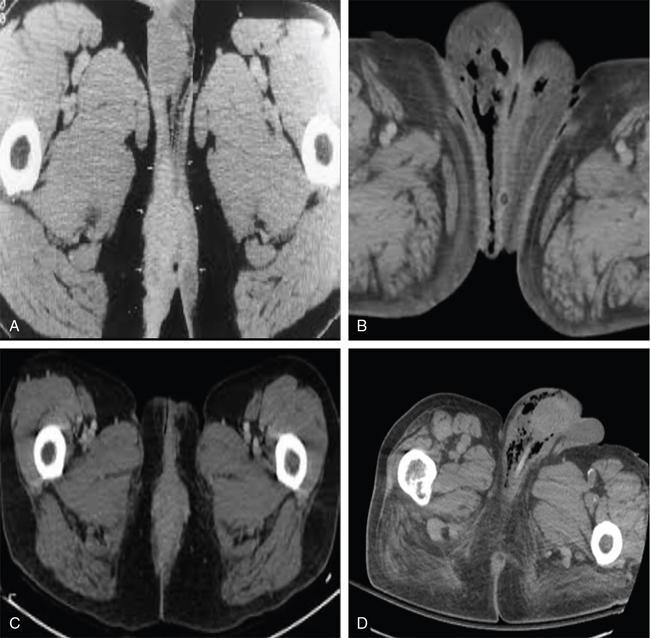
CT scan
MRI scan
Treatment
Complications
Treatment outcome
Prognosis
Lair’s fournier’s gangrene severity index (FGSI)
New prognostic criteria for fournier’s gangrene
Prevention
Conclusion
Abdominal wall hernias
Ultrasound techniques and appearance
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Scrotum
11.11.1
11.11.2






