Anidudha Kulkarni Seminal vesicles (SVs) are an integral part of male genitourinary system. SVs are paired accessory gland which plays a major role in male fertility. They produce an alkaline fluid contributing 50%–80% of the ejaculate volume. Male genital organs collectively work to produce semen, consisting of mature spermatozoa. There are no specific signs and symptoms for pathologies in SVs. The common complaints include pain, recurrent UTI and dysuria. Commonly, an abnormality is identifies while investigating for an unrelated pathology such as infertility or a prostatic nodule. SVs are paired organs, measuring 5–7 cm in length, which are rounded superiorly and taper inferiorly. SVs are located posterior to the bladder and inferolateral to the vas deferens. This bilateral positioning of the SVs creates a ‘V’-shaped configuration. SVs are positioned superior to prostate. They lie at the inferior aspect of the rectovesical pouch. SV ducts merge with ampulla of vas deferens and form the ejaculatory duct which opens into the prostatic urethra at the level of verumontanum. SVs contain highly granular cells that produce straw coloured alkaline fluid containing fructose, proteins and vitamin C under the influence of testosterone. The fructose provides the required energy for the motility of spermatozoa. This fluid makes up two-thirds of the total ejaculate volume. Rest of which comes from the prostate gland, vas deferens and lesser amounts from bulbourethral and Cowper’s glands. SVs appear as fluid-filled structures, with a thin septations on contrast-enhanced CT. This modality remains helpful in recognizing many SV abnormalities. On MRI they show low signal intensity on T1-weighted and high signal intensity on T2-weighted images and appear as elongated fluid-filled structures with thin septae. SVs appear as symmetric organs which lie cephalad to the prostate and posterior to the bladder They have a typical ‘bow-tie’ appearance in transverse scans and a club or tennis-racket shape in longitudinal scan. They show homogenously fine echoes, however they are less echogenic than prostate. SV volume is positively affected by circulating testosterone and prolactin, and increases during a prolonged sexual abstinence. Volume of SVs tends to shrink after the fifth decade. SV agenesis is a rare congenital anomaly with an incidence of 0.08%, where there is a complete or partial absence of one or both SVs. This anomaly results in infertility secondary to azoospermia. Patients are generally asymptomatic. Only symptom is infertility and thin low volume ejaculate. TRUS remains the modality of choice to diagnose patients with SV agenesis. There is no treatment available for the SV agenesis. The ureteric bud develops from the mesonephric duct during the 5th week of intrauterine life. In the 7th week, the testes develop and differentiate the male genital system. SVs develop as a bulbous swelling of distal portion of mesonephric duct during the 12th week of gestation. SVs are retrovesicle to the urogenital sinus. SV agenesis is often associated with abnormal development of other mesonephric/metanephric derivatives, such as the VD, ureter and kidney. Unilateral SV agenesis is due to insult occurring before the 7th week of gestation, when the ureteric bud arises from mesonephric duct. Bilateral SV agenesis is related to CFTR gene mutations (64%–73% of cases). A decreased SV volume is defined as hypoplasia, and mainly refers to congenitally small SV, although an acquired form may be associated with testosterone deficiency or postinfective scarring. The normal SV measures >25 mm in length. They are considered to be hypoplastic when >16 mm but <25 mm and atrophic when <16 mm Another parameter which can be considered for hypoplasia is the maximum anteroposterior diameter being smaller than 50% of normal or <5 mm. Hypoplasia of the SVs may be unilateral or bilateral. This condition usually is associated with other genitourinary anomalies such as absence of the ipsilateral vas deferens and ejaculatory ducts.
11.10: Seminal vesicles
Anatomy
Physiology
Imaging

Computed tomography
Magnetic resonance imaging
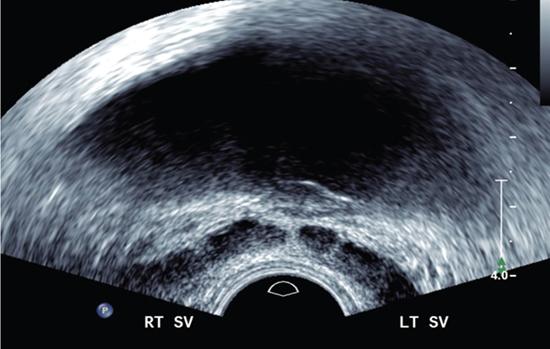
Trus
Diseases of the seminal vesicles
Seminal vesicle agenesis
Embryology

Seminal vesicle hypogenesis
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


