Breast magnetic resonance imaging (MRI) was introduced into the breast imaging community in the 1990s. A considerable number of research studies were conducted, with findings revealing promising results Breast MRI provided a novel approach to detecting breast cancer and diagnosing additional unsuspected breast lesions alongside the standard mammography technique. Implementation of breast MRI now was being considered by facilities as an additional imaging modality.
Published breast MRI research has shown 94% to 100% sensitivity in diagnosing invasive cancer, with a lower sensitivity of 40% to 100% for ductal carcinoma in situ (DCIS). A study by Zakhireh and colleagues showed a sensitivity of 95% in detecting breast cancer when mammography and breast MRI were combined for screening women at high risk of developing cancer. Such literature supports implementing breast MRI into a practice because it has the ability to enhance services provided to patients. However, adding breast MRI is a major undertaking. This chapter will be based on our experience of implementing breast MRI in our practice, which is located in western New York in the city of Rochester. We are an outpatient breast imaging center founded in 1976 that currently staffs approximately 130 employees. We offer a wide range of services to our patients: mammography, bone densitometry, ultrasonography, ductography, needle biopsy, and breast MRI. We see approximately 80,000 patients and diagnose approximately 650 cancers annually. Our facility has evolved over the years to continue to provide the latest technology and offer the best care to our patients. This chapter will discuss our experience and the importance of adequate planning and education to optimize and minimize the challenges that may occur when incorporating breast MRI into your practice.
Existing Practice Needs
Initially, when breast MRI is added, the needs of the facility must be considered. This section will discuss many of the topics that should be addressed before purchase.
Once the decision is made to incorporate breast MRI into the practice, it is beneficial to assign either an individual or a group of staff members to perform the initial research. A search should be conducted of equipment (magnets and coils) available on the market: What is out there? What are the costs? Many options are available, including purchasing equipment that is new or refurbished, as well as leasing the equipment. Based on a facility’s particular practice setting, one of these options will be the most optimal. Vendors can present various choices that meet the needs and specifications of the site. The vendor may also provide beneficial business information, such as the number of imaging procedures needed to pay for the equipment. This information will give a site’s manager the ability to compare vendors and help make purchasing decisions that will best fit the practice.
Community Research
Some medical communities have boards that have been created to ensure that patients have access to beneficial technology while minimizing increasing community costs. In our community of Rochester, located in western New York, this board is called the Community Technology Assessment Advisory Board (CTAAB). Such boards are made up of individuals representing the business and insurance community, consumers, physician groups, health systems, and other community groups. Initially, a site’s officials may have to plead their case as to why a particular modality is essential to their practice. An application providing all information regarding equipment (proposed use, staffing, projected costs, and revenue) and an oral presentation of the proposal are usually required. This process can be lengthy and time intensive, but it is essential for a positive outcome that due diligence are given. To provide evidence for the proposal, published research on using breast MRI will need to be incorporated in the application and presentation. If the board grants approval, the site will be able to move forward with implementation.
Patient Referral Base
Concerns that should be addressed to help assess the initial patient needs of the practice include the following:
- •
How large is the breast imaging practice? What percentage of the practice’s work is for breast imaging?
- •
What type of patients will be referred to breast MRI: newly diagnosed breast cancer patients, high-risk patients, patients with an inconclusive work-up?
- •
How many cases of breast cancer are diagnosed at the facility?
- •
Does the practice serve a high-risk population? If so, what services have been put into place to identify those at risk? Is there a genetic counseling program with risk assessment available?
- •
Will the magnet be used for breast imaging only or will it be used for whole body imaging as well?
- •
How will the practice communicate with and educate referring physicians about the new breast MRI program?
Initial Investigation
Before a purchasing decision is made, the benefits and shortcomings of the available options must be diligently explored. Conversations with experienced breast MRI personnel and visits to their practices will be very beneficial to the decision-making process (as it was in our experience), especially if MRI is new to the physicians and staff. These actions will help site officials make the best decisions for the facility and for its patients.
Facility Limitations
Personnel at breast centers that have no MRI experience should take the opportunity to learn all they can about MRI safety. A good place to begin is to consult the American College of Radiology’s (ACR) guidance document on MRI safety. This document provides guidance and sample diagrams for the design of a safe MRI suite; it is crucial that safety be incorporated into its infrastructure. The ACR recommends four safe zones, with zones three and four having the strictest access. These zones are restricted and controlled by MR personnel and are physically restricted by passkey locking systems, key locks, and so on. Our facility uses a passkey locking system, which we have found has elevated the level of security. This system provides a much more secure environment because only key personnel know the passkey, ensuring that those who are not authorized cannot gain access. When designing a suite, a project manager from the MRI vendor familiar with executing an MRI safe design will most likely be involved.
Space is a big consideration in the installation plan for an MRI suite. It must be determined whether the facility has existing space available, will need an addition to the building, or will need to acquire additional department space. Each MRI unit on the market will have its own room specifications. Other important areas associated with the MRI examination that need to be created are as follows: patient changing rooms, nurse station for IV access, technologist control room, patient reception and waiting area, storage room, and bathrooms. If a facility has to build an addition to an existing structure, building codes will need to be addressed and an architect hired. If space is limited, a dedicated breast MRI magnet may be an option to explore because this type of unit is smaller than a whole body magnet. Another option if space is limited is to lease a mobile unit. This is especially beneficial if the referral base is unknown or if a low number of referrals is expected initially.
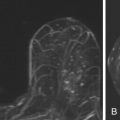
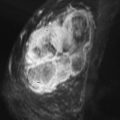
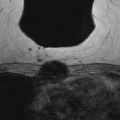
Our first experience with breast MRI was with a leased 1.5 Tesla (T) General Electric mobile unit, staffed with a certified MRI technologist, one day a week ( Figure 1.1 ). This initial choice best minimized our risks, allowed us to incorporate the modality gradually, and allowed our staff to ease into MRI training while learning the technology firsthand. Within 2 years of initiation of our breast MRI practice, we needed more days to accommodate the patients, and this eventually grew to a full-time need. Because of this, we decided to build the addition to the building for the MRI suite that exists today.

Magnets and Breast Coils
Most sites use a magnet of at least 1.5 T in field strength to allow for the necessary speed and spatial resolution for breast MRI. It may be wise to consider that vendors are now making available 1.5 T magnets with larger bores, for accommodating larger patients.
A variety of coils are on the market and it may be beneficial to have more than one to accommodate different breast sizes. The coils should allow access to the breast for routine image positioning as well as for interventional procedures. For biopsies and localizations, it is essential to have a coil that will provide both lateral and medial access. However, it is just as important to look at the posterior access: how close to the chest wall can you get with a certain coil? The breast coil is an expensive purchase and is crucial in regards to image quality, so it is important to fully explore the options, features, and limitations of the products available. Listed below are some considerations when choosing breast coils:
- •
How comfortable is the coil? Have the vendor bring a sample coil for a demonstration to your facility. Have volunteers of different body habitus lie on it in the same position that would be used for the MRI. An uncomfortable patient will move and impair image quality.
- •
Is the breast coil easy to use? Are the moving parts easy to operate? Are they robust enough to hold up to daily use? Will they clean well after procedures?
Sixteen-channel coils have recently been introduced for optimizing signal-to-noise ratio. Some of these are designed with a closed cup construction, which surrounds the breast tissue, for best signal. This can make positioning a challenge, and a separate coil is used for biopsy. Others have coil elements built in to the compression paddles, which allows the elements to be customized to each patient. For biopsy with this construction, the paddle element is switched for a biopsy immobilization grid, thus turning the coil effectively into a seven-channel coil for the biopsy procedure.
Power Injector
Another piece of equipment that requires consideration is a power injector. When we first began breast MRI imaging, our nurse injected the contrast by hand. Our injection rate is 2 mL/second, with a 30 mL saline flush, also at 2 mL/second. Allowing true confidence in the consistency of the timing, a power injector will ensure that the injection is the same for every patient, every time. This is important for two reasons. First, the kinetic data gathered after the patient is injected is entirely dependent on timing. Second, many patients come for scanning on an annual basis and interpretation of a change on the MRI study from previous years is complicated when there is the possibility that variation may be due to differences in the injection rate. Using a power injector will remove this variable.
Our most noticeable change after we began using the power injector was that our patients moved less during injection, probably because the nurse no longer was injecting by hand. Minimizing patient movement led to better studies.
Implementing Breast Magnetic Resonance Imaging
Magnetic Resonance Imaging Staff
Patients that are referred to breast MRI have individualized concerns that need special considerations. Those being referred for an MRI to evaluate the extent of the disease are extremely anxious because of the recent diagnosis of breast cancer. Women who are at high risk of developing breast cancer or women with an inconclusive mammographic work-up will have increased anxiety as well, fearing the possibility of a finding that may be cancerous. Before the procedure, the physician should inform the patient of why the examination is being recommended as well as what might result from the procedure, such as follow-up MRI examinations or the need for an MRI biopsy.
Having dedicated scheduling staff is beneficial because they will be well versed in the specific needs of breast MRI patients. In our facility, two dedicated staff members assist patients with insurance preauthorization, scheduling, and patient check-in. Additionally, they inform patients about the examination—the length of time it will take and how to prepare—and inform them about the contrast injection. These trained staff members will discuss MRI contraindications, such as implantable devices and claustrophobia, and conduct a health-history survey that includes questions regarding prior contrast reaction, date of last menstrual cycle, and hormone use ( Figure 1.2 ). This approach has helped minimize patient stress and, most important, gives the patient a contact person because many times this will be the first person the patient meets when arriving for the appointment. An information packet is sent through the mail before the appointment date; this includes much of the information covered over the phone by the MRI staff member ( Figure 1.3 ).