Sinonasal Adenocarcinoma
Michelle A. Michel, MD
Key Facts
Terminology
Malignant neoplasm with glandular differentiation, or arising from surface epithelium or minor salivary rests
Imaging
Predilection for nasal cavity & ethmoid sinuses
May reach large size due to delay in diagnosis
75% with involvement of > 1 SN area at diagnosis
CT
Well- to poorly defined soft tissue density mass
Bone destruction > remodeling
MR
Typically intermediate to hyperintense T2 signal
Diffuse, heterogeneous enhancement
Top Differential Diagnoses
Sinonasal squamous cell carcinoma
Esthesioneuroblastoma
Sinonasal undifferentiated carcinoma
Sinonasal non-Hodgkin lymphoma
Pathology
Confusion remains regarding histologic classification of sinonasal adenocarcinoma
2 major subtypes
Intestinal (related to wood dust exposure): Most frequent form colonic > solid > papillary > mucinous & mixed type
Nonintestinal: Unrelated to wood dust exposure
Accounts for 15% of all SN cancers
Clinical Issues
6th decade most common
M > F (≈ 3:1)
Poor prognosis with higher grades, incomplete resection, & intracranial involvement
Complete surgical excision for cure
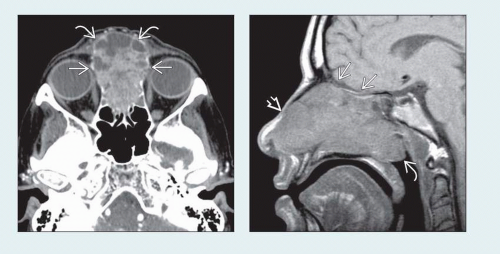 (Left) Axial CECT shows a large, heterogeneously enhancing adenocarcinoma filling the upper nasal cavity and ethmoid sinuses. There is anterior extension into the soft tissues of the nasal dorsum
 and destruction of the lamina papyracea and destruction of the lamina papyracea  . (Right) Sagittal T1WI MR shows a large adenocarcinoma filling the nasal cavity and extending into the nasopharynx . (Right) Sagittal T1WI MR shows a large adenocarcinoma filling the nasal cavity and extending into the nasopharynx  . No extension through the skull base . No extension through the skull base  is seen. The lesion extends into the subcutaneous fat is seen. The lesion extends into the subcutaneous fat  anteriorly. anteriorly.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|