SINONASAL PRIMARY BONE ORIGIN TUMORS
KEY POINTS
- Computed tomography can be highly specific in the diagnosis of the rare occurrence of primary craniofacial bone tumors.
- The mandible typically is more likely to be involved by some of these tumors than the sinuses and nasal cavity.
- Cystic varieties of these lesions without identifiable matrix usually cannot be distinguished from one another with imaging and will often fail if curettage is the chosen definitive therapy; thus, imaging extent greatly impacts medical decision making if a gross bony margin must be taken.
- In malignant forms of these tumors, imaging must include an assessment of perineural spread and sometimes regional lymph node spread and distant disease.
TUMOR TYPES: GENERAL CONSIDERATIONS AND DIFFERENTIAL DIAGNOSIS
Tumors of bone origin may come from one of several cell lines, and more than one line of differentiation may be present in any particular benign or malignant bone tumor. These arising may be of fibro-osseous, dental, chondroid, osteoid, and osteoclastic origin. The general growth patterns and imaging appearance of these primary bone tumors are discussed in detail in Chapters 38 through 42. The sinonasal region manifestations of those tumors arising from osteocytes, chondrocytes, and osteoclasts are discussed in summary in this chapter. Fibro-osseous sinonasal tumors are discussed in Chapter 91, and dental-related tumors are discussed in Chapter 99. Systemic diseases that arise from elements predominantly in the marrow space of the craniofacial skeleton are discussed in Chapter 92 along with craniofacial bony metastatic disease.
Osteoma
Osteomas are benign and very common. They are typically of no clinical consequence, being seen only as incidental findings on studies done to evaluate unrelated symptoms of sinus and nasal cavity disease (Fig. 38.3A). Osteomas arise most commonly from the paranasal sinuses when they occur in the head and neck region, predominantly in the frontal and ethmoidal sinuses. Some can grow to very large size and project into the orbit or cranial vault (Fig. 90.1). Rarely, these lesions can carry or displace bits of mucosa into these sites, causing a very unusual displaced secondary mucocele (Figs. 38.3, 85.6, and 90.2).
Large or smaller but strategically located osteomas might obstruct the sinonasal drainage pathways (Fig. 83.9C). This can result in chronic sinusitis or even a mucocele that would require surgery to remove the osteoma in order to deal with the postobstructive changes (Figs. 38.3B, C and 90.2).
Osteomas may be associated with Gardner syndrome (Fig. 90.3).
Osteogenic Sarcoma and Osteoblastoma
Osteogenic sarcoma is the most common malignant primary tumor of bone. It presents most frequently in the second decade of life. Predisposing factors include prior radiation (Figs. 38.8, 38.9, and 90.4), Paget disease, fibrous dysplasia, and chronic osteomyelitis. Osteoblastoma is very rare, and its matrix may appear more like that of a cartilaginous or fibrous lesion (Fig. 38.6)
Osteosarcoma is rare in the sinuses since the most commonly affected facial bone is, by far, the mandible. The maxillary is the most commonly affected sinus. Ethmoid and sphenoid bone osteogenic sarcomas are extremely rare. Prior radiation treatments to the craniofacial region, especially in childhood, considerably raise the risk of this disease. In fact, sinonasal osteosarcoma is distinctly rare in the absence of a history of prior radiation (Figs. 38.8, 38.9, and 90.4). Most are high grade.
The ossifying matrix of an osteogenic sarcoma may suggest a meningioma or even fibrous dysplasia as an initial diagnostic consideration. A juvenile ossifying fibroma of the maxilla may also raise the concern for a rare maxillary osteogenic sarcoma (Chapter 91). Mucinous minor salivary gland cancers or metastases that calcify might mimic an osteogenic sarcoma.
Chondroma
Chondromas are rare tumors that arise from the cartilaginous portion of bones formed by enchondral ossification. In the sinonasal region, the nasal septum as well as the bones of the skull base and paranasal sinuses are most likely to be the source of these tumors. Typical matrix calcification, when it occurs, makes the diagnosis relatively easy to anticipate. Most of these are lesions that when encountered will be finally diagnosed as a low-grade chondrosarcoma (Fig. 39.1).
Chondrosarcoma
Chondrosarcomas arise from enchondral bones. Sinonasal-region lesions tend to arise from the central skull base or paranasal sinuses. The nasal septum within the nasal cavity is another potential site of origin of these rare lesions (Figs. 39.1 and 90.5). As with chondromas, a typical matrix calcification, when it occurs, makes the diagnosis relatively easy to anticipate; however, a morphologically heterogeneous matrix without typical “rings and stipples” may suggest an osseous or mineralizing fibrous matrix or a chondroid variant such as chondromyxoid fibroma (Figs. 39.11, 90.6 and 91.5).
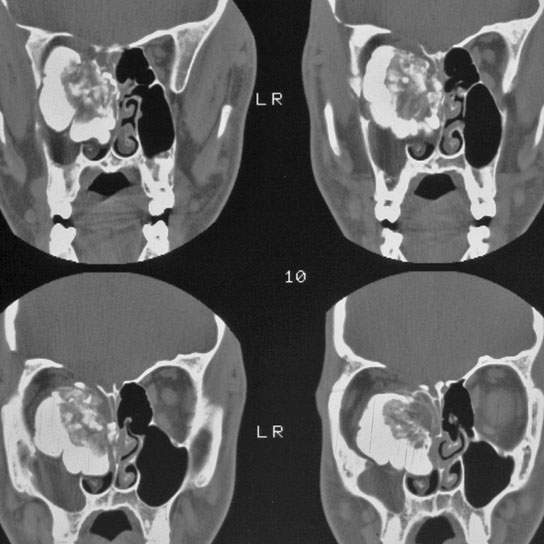
FIGURE 90.1. Four images showing the extent of a very large osteoma that arose in the nasal cavity but grew to severely affect the orbit and anterior skull base.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


