SINONASAL SYSTEMIC MALIGNANCIES
KEY POINTS
- One must recognize the patterns of the sinus and nasal cavity diseases discussed in this chapter to avoid unnecessary patient morbidity.
- Recognizing such disease at the time of initial presentation is often difficult but may be aided greatly by the presence of noncontiguous multifocal disease or atypical spread patterns.
- The nature of necrotizing nasal cavity masses is currently understood much better than in previous years, and many of these processes are now known to be manifestations of lymphoma. Aberrancies in naming of these diseases still persist and should be removed from the clinical lexicon.
TUMOR TYPES: GENERAL CONSIDERATIONS AND DIFFERENTIAL DIAGNOSIS
The vast majority of sinonasal cancers are of epithelial origin (Chapter 89). The differences between those cancers and the ones presented in this chapter are most often very substantial with regard to medical decision making, especially treatment options. Modern pathologic evaluation including immunohistochemistry and tumor immunophenotyping only occasionally leaves the diagnosis in question once sufficient tissue has been obtained. However, failure to recognize the patterns of the sinus and nasal cavity diseases discussed in this chapter can lead to unnecessarily morbid approaches to tissue sampling and even attempted unnecessary gross total excision.
The diseases are recognized by how their spread patterns differ from other sinonasal cancers. The biggest clue is multifocal disease, followed closely by a pattern that suggests a bone or bone marrow origin of the disease. When these cancers present as a solitary mass, their true nature is usually not apparent until the tissue is sampled.
The tumor types that will generally be under consideration in this spectrum of sinonasal disease are discussed in the following sections. The differential diagnosis may include chronic fungal and other infections that cause skull base osteomyelitis (Chapters 86 and 115). Also, the noninfectious granulomatoses and histiocytoses and, rarely, pseudotumor will enter the initial diagnostic thought process (Chapter 87); these usually need to be excluded by some combination of clinical evaluation, imaging and laboratory findings, and ultimately tissue sampling.
Lymphoma and Leukemia
The general pathophysiology of lymphoma, leukemia, and related diseases are discussed in Chapters 26 through 28. Sinonasal lymphoma may affect the very young but more frequently occurs in middle-aged and older men (Figs. 92.1 and 92.2). Occurrences of such disease are almost exclusively non-Hodgkin lymphoma, and most sinonasal presentations herald stage 4 disease requiring a systemic workup with imaging, laboratory studies, and often bone marrow biopsy. Children respond better to chemotherapy than adults. Relapse drops ultimate survival rates precipitously.

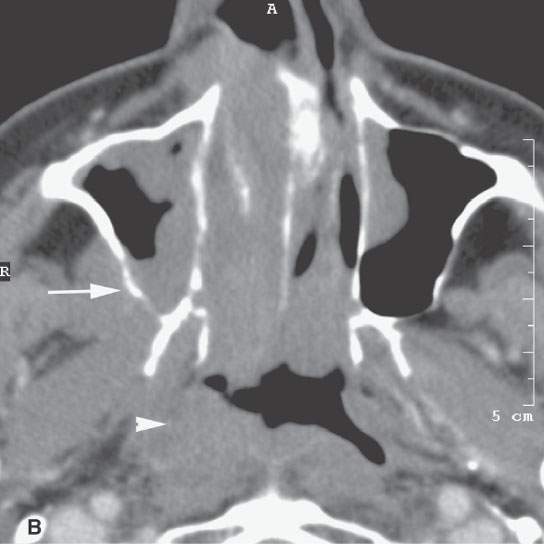
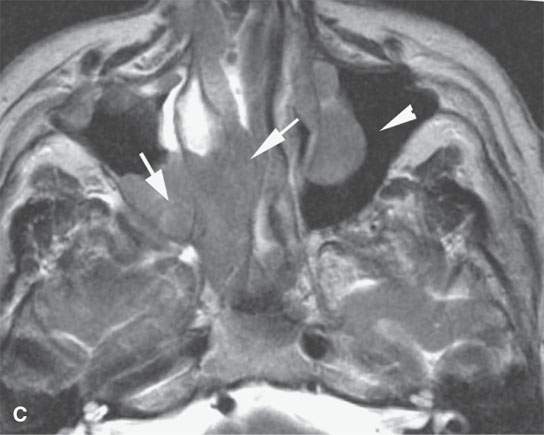
FIGURE 92.1. Computed tomography (CT) and magnetic resonance (MR) study of a patient with lymphoma of the sinus and nasal cavity and a second patient with posttransplant lymphoproliferative disorder (PTLD). A–F: Patient 1. In (A), CT shows a mass invading the anterior ethmoids from the anterior nasal cavity (arrow) with extension into the orbit (arrowhead) but no invasion of orbital fat. In (B), CT more inferiorly shows tumor throughout the nasal cavity but also invading through the posterior wall of the maxillary sinus (arrow) and a separate area of invasion in the nasopharynx (arrowhead). In (C), the T2-weighted (T2W) image shows contiguous disease in the left nasal cavity and maxillary sinus (arrows) with a noncontiguous focus of disease in the left maxillary sinus (arrowhead). In (D), another noncontiguous focus of disease seen on the CT study in (B) is confirmed in the nasopharynx (arrow). (NOTE: Multifocal areas of involvement and involvement of the Waldeyer ring strongly suggest the diagnosis of lymphoma.) In (E), the contrast-enhanced T1-weighted image shows noncontiguous areas of disease in both maxillary sinuses and in the ethmoid sinus (arrows) and a suggestion of perineural spread along the right infraorbital neurovascular bundle (arrowhead). Multifocal disease suggests a systemic malignancy. In (F), there is additional invasion of the epidural space, confirming the suspicion of lymphoma presenting as a sinonasal mass, with the proper diagnosis being suspected on the basis of the imaging pattern of disease. G, H: Patient 2. MR study of a transplant patient with nasal congestion. In (G), the T2W image shows an infiltrating process in the high posterior nasal cavity and ethmoids and sphenoid (arrows) with involvement of the cavernous sinus (arrowhead). The black arrows show bilateral mastoid and middle ear mucosal thickening due to involvement of the nasopharynx seen in the next image. In (H), the T2W image shows noncontiguous disease in the left maxillary sinus and likely involvement of the nasopharynx manifest as what appears to be lymphoid hyperplasia that is not obviously invasive (arrows). (NOTE: The multifocal nature of this disease again suggests possible systemic malignancy. In this case, PTLD was confirmed by elevated Epstein-Barr virus titers and response to therapy cessation.)
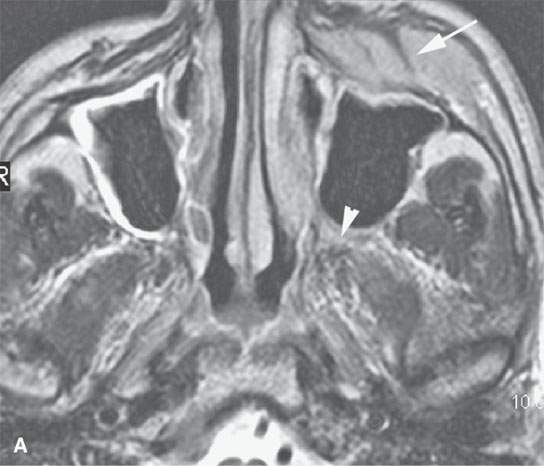


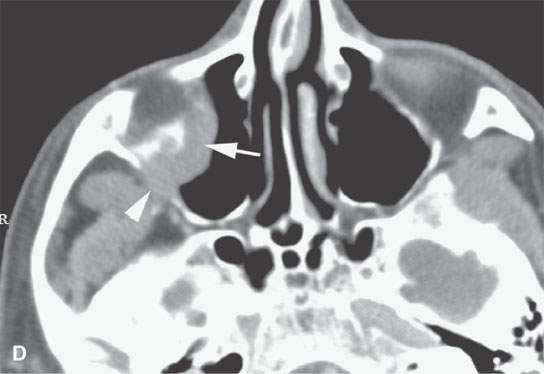
FIGURE 92.2. Systemic lymphomas can sometimes have unusual patterns of presentation as illustrated by these four patients. A: Patient 1. T2-weighted magnetic resonance imaging shows an infiltrating mass deep to the superficial musculoaponeurotic system in the region of the canine fossa (arrow) with evidence of perineural spread to the pterygopalatine fossa. The combination of mass in this location likely is due to involvement of infraorbital facial nodes, and perineural spread strongly suggests lymphoma as the proper diagnosis. B: Patient 2. Computed tomography showing bilateral nodular masses in the canine fossa region on both sides (arrows). On the right, the disease obviously infiltrates bone and spreads to the nasal cavity. The multifocal nature of disease and propensity to occur in the canine fossa likely is related to the infraorbital nodes of the facial group being in this location. C: Patient 3. A patient with an infiltrating frontal sinus mass suspected clinically of being an epithelial malignancy. The behavior is somewhat unusual with regard to its infiltrative pattern and leaving areas of residual bone along the outer table behind (arrows); this would be unusual for epithelial malignancy. This was proven to be lymphoma of the frontal sinus. D: Patient 4 presented with facial pain on the right side. An infiltrating mass was noted in the maxillary sinus (arrow). The finding of aggressive behavior is related to destruction of the posterior sinus wall with invasion of fat retroantral (arrowhead). The unusual spread pattern raises the possibility of lymphoma, although this is a nonspecific finding.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Oropharynx: Introduction
Oropharynx: Introduction
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


