30 Small bowel obstruction
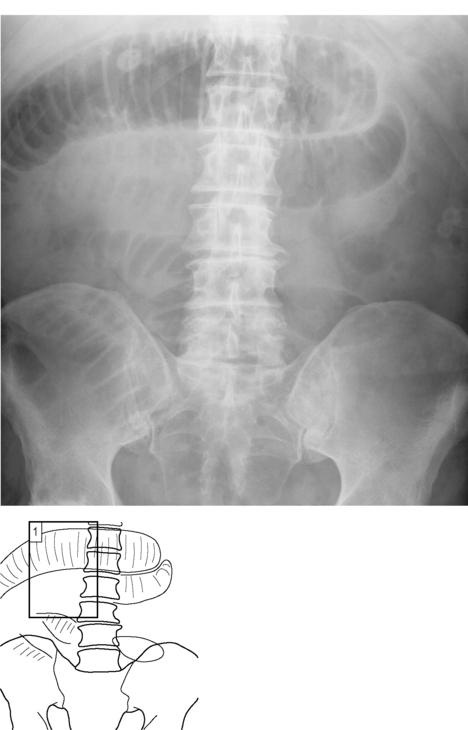
Fig. 30.1A The radiograph shows several abnormally dilated small bowel loops in small bowel obstruction.
Background
Be aware of the complication of perforation – longstanding small bowel obstruction leads to bowel ischaemia and necrosis which may initially manifest as pneumatosis intestinalis (see Chapter 37). Do not forget to request an erect CXR in patients with suspected obstruction and look for the signs of perforation (see Chapters 27 and 45).









