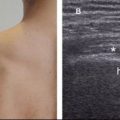
Figure 10-3. Incomplete tear at the musculotendinous junction of the pectoralis major. [A] Positioning of the probe. [B] Corresponding 12-5 MHz US image depicts an  incomplete tear (asterisks) located at the musculotendinous junction of the pectoralis major tendon (arrowheads). Delt= deltoid. Gt= greater tuberosity.
incomplete tear (asterisks) located at the musculotendinous junction of the pectoralis major tendon (arrowheads). Delt= deltoid. Gt= greater tuberosity.
Non-surgical treatment is currently reserved for incomplete or intramuscular tears, especially those affecting elderly or other lower demand individuals.7 In the remaining, early repair is usually recommended, highlighting the importance of awareness of this injury.8
3.2. Myositis Ossificans
Aberrant repair of muscle injury may result in calcification, a condition first described by French doctor Guy Patin in 1692.9 Two centuries later, Von Dusch coined the term myositis ossificans.10 The term is still the most popular descriptor for the pathology, though recent evidence indicates that the condition is not predominantly inflammatory as suggested by the suffix –itis. Based on its clinical and histological features, myositis ossificans is currently considered a benign reactive pseudosarcomatous lesion.11 Most cases are observed in young individuals as a result of trauma, though the condition sometimes occurs without a definite identifiable cause.
Calcification typically occurs within 2 to 6 weeks after injury,14 and is seen 2 weeks earlier at US when compared to radiographs.15 The lesion develops in distinct stages with different presentations at US. In the early stage, termed immature, US depicts a non-specific soft tissue mass that ranges from a hypoechoic area with an outer sheet-like hyperechoic peripheral rim12 to a highly echogenic area with variable shadowing.13 In the late stage, termed mature, myositis ossificans is depicted as an elongated calcific deposit that is aligned with the long-axis of the muscle, exhibits acoustic shadowing, and has no soft tissue mass associated (figure 10-4). US may suggest the diagnosis at early stage, but imaging features need to evolve with successive maturation of the lesion and formation of the characteristic late stage changes before they become pathognomonic. On CT and MRI, late stage myositis ossificans may show a characteristic zonal phenomenon, composed of immature bone formation in the center of the lesion surrounded by a dense zone of mature ossification at the periphery.
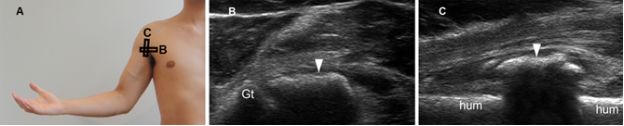
Figure 10-4. Late stage ossifying myositis. [A] Positioning of the probe. [B] Corresponding long-axis 12-5 MHz US image depicts an elongated calcific deposit that is aligned with the pectoralis major muscle (arrowhead). [C] Corresponding short-axis 12-5 MHz US image confirms the shadowing calcific deposit. Gt= greater tuberosity. Hum= humerus.
The differential diagnosis includes many tumoral and nontumoral pathologies. A main concern is to differentiate early myositis ossificans from malignant soft-tissue tumors, and the latter is suggested by a fast-growing process. The full course of growth of myositis ossificans is about 7-8 weeks from inception, and this information can be used to reassure diagnosis and judge whether the ossification is mature or not in order to reduce the risk of recurrence after surgical intervention.16 If clinical or imaging findings are dubious and extraosseous sarcoma is suspected, biopsy should be performed.17 At histology, detection of the typical zonal phenomenon is diagnostic of myositis ossificans,18 though microscopic findings may be misleading during the early stage.19
3.3. Hypoplasia and Agenesis
Hypoplasia and agenesis of the pectoralis major muscle are typically observed as a part of Poland syndrome, named after English surgeon Alfred Poland.20 Although several theories have been advanced to explain the pathogenesis, the most widely accepted evidence indicates that it results from hypoplasia of the subclavian artery during the sixth week of gestation.21 The critical event occurs when the medial and forward growth of the ribs damages the subclavian artery, resulting in a cascade of developmental abnormalities in the areas supplied by this artery. The specific region of vessel involvement and degree of flow impairment dictate the extent and severity of the syndrome.22,23 Although clinical picture varies, the sine qua non of Poland syndrome is hypoplasia of the sternal and abdominal heads of the pectoralis major muscle. Most cases arise sporadically, with no familial predisposition. Because the functional disability is usually mild, patients seek medical assistance mainly for aesthetic reasons. The diagnosis is usually obvious at clinical examination, but US can also document the classic finding (figure 10-5).
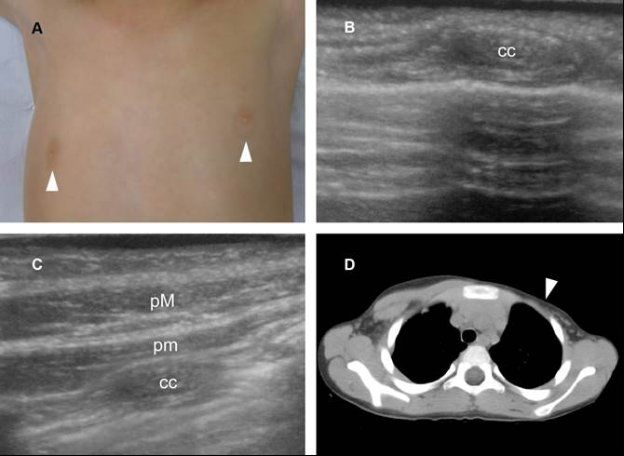
Figure 10-5. Pectoralis muscles agenesis. [A] Clinical presentation. Note asymmetric positioning of the nipples (arrowheads). [B] Sagittal 12-5 MHz US image confirms clinical diagnosis of left pectoralis muscles agenesis. [C] Comparative contralateral sagittal 12-5 MHz US image shows normal pectoralis major (pM) and minor (pm). [D] Corresponding CT confirms pectoralis muscles agenesis in the left side (arrowhead). Cc= costal cartilage.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


