Spine Trauma and Degeneration
Gaurav Jindal
Prachi Dubey
Rafeeque Bhadelia
QUESTIONS
1 Patient s/p MVA.
 Images courtesy of Dr. Nafi Aygun |
1a What is the best description for the pattern of injury shown?
A. Chance fracture
B. Compression fracture
C. Burst fracture
D. Avulsion fracture
1b Which of the following is associated with the above injury?
A. Mechanically stable injury without any associated injuries
B. Most patients have significant neurologic injury.
C. Commonly associated with visceral injuries
D. Extreme hyperextension resulting in dorsal soft tissue injury
View Answer
1b Answer C. Commonly associated with visceral injuries. Images courtesy of Dr. Nafi Aygun
|
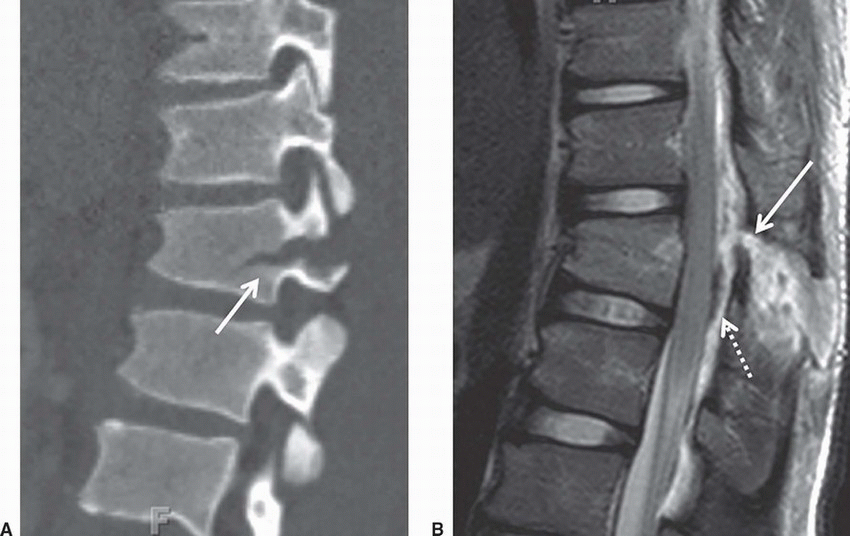
Imaging Findings: Sagittal CT image shows a transverse fracture through the vertebral body and pedicle, (arrow A). Sagittal T2 weighed MRI shows disruption of the ligamentum flavum, (arrow B), adjacent interspinous edema and widening. Note there is also a dorsal epidural hematoma, (dotted arrow).
Discussion: Chance fracture is an unstable injury characterized by horizontal splitting of the spinal canal resulting from a flexion distraction mechanism. It may involve the osseous and/or discoligamentous complex. It is most commonly seen at the thoracolumbar junction. On radiographs, distraction of the posterior elements results in an “empty body” sign on frontal view due to displacement of the spinous process from its normal position. On CT, a transverse split of the spinal column is seen as a fracture line through the posterior elements often with extension into the vertebral body.
Anterosuperior compression fractures of the vertebral body are also commonly associated. Burst vertebral fracture morphology may also be seen (Chance-burst fracture).
MRI can better delineate posterior ligamentous complex injury as well as identify any cord damage. Although mechanically unstable, patients seldom have neurologic deficits at presentation. Intra-abdominal injuries especially involving the bowel and mesentery have been reported in up to 40% of cases and must be closely sought in patients with a Chance-type fracture.
References: Bernstein MP, Mirvis SE, Shanmuganathan K. Chance-type fractures of the thoracolumbar spine: imaging analysis in 53 patients. AJR Am J Roentgenol 2006;187(4):859-868.
Dane B, Bernstein MP. Imaging of spine trauma. Semin Roentgenol 2016;51(3):180-202.
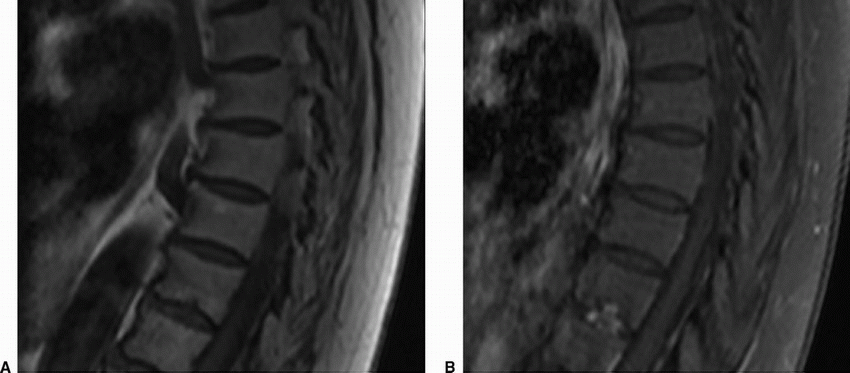
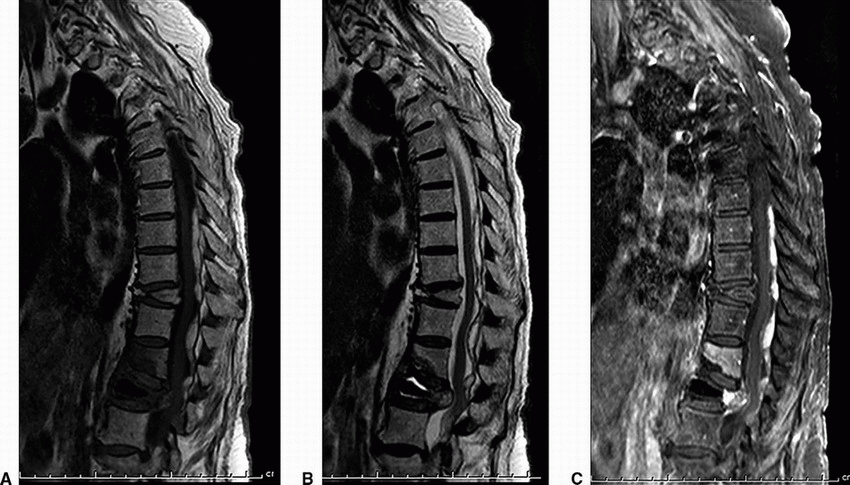
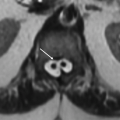
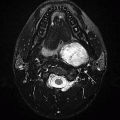
2 A 50-year-old woman with acute midthoracic back pain presented to the ER. An MRI was performed with intravenous contrast; key images are shown below.
|
2a Further clinical workup did not reveal any signs of symptoms to suggest infection. What is the most likely diagnosis?
A. Acute Schmorl node
B. Discitis/osteomyelitis
C. Disc metastasis
D. Intraosseous hemangioma
View Answer
2a Answer A. Acute Schmorl node. This study shows endplate edema involving the central and posterior aspect with corresponding enhancement. Note relatively rounded nodular morphology invaginating along the endplates on the pre- and postcontrast T1w sequences, typical for Schmorl node formation. Often, the appearance can be indistinguishable on imaging from discitis/osteomyelitis especially early in the disease course, and therefore, interpretation in the clinical context is very important.
2b Which of the following disorders is associated with the above condition in younger individuals?
A. Mucopolysaccharidoses
B. Ankylosing spondylitis
C. Scheuermann disease
D. Renal osteodystrophy
View Answer
2b Answer C. Scheuermann disease. A condition of abnormal kyphosis typically seen in the thoracic spine in the prepubertal age group, it has been associated with multiple endplate Schmorl node formation. The other conditions also have skeletal manifestations, but none of them have a specific predisposition toward Schmorl node formation.
|
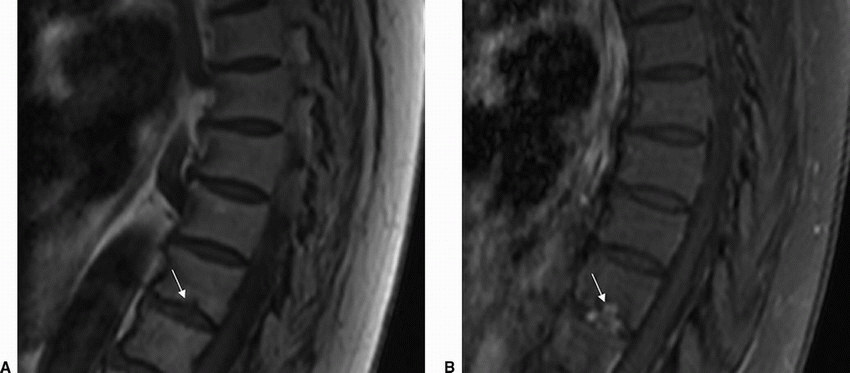
Imaging Findings: Sagittal pre (A) and post contrast T1w image (B) shows herniation of disc material through the inferior endplate (arrow A) with corresponding enhancement (arrow B). This is compatible with acute Schmorl node formation.
Discussion: Schmorl nodes are disc herniations into the endplates, either into the weakened cartilaginous endplates or within the subchondral bone. The weakened zones provide least resistance to expansion of the nucleus pulposus especially in younger individuals with intact annulus fibrosis. The herniated material typically comprises the nucleus pulposus with associated degenerative or inflammatory response. In the chronic phases, there is characteristic sclerosis along the abutting vertebral spongiosa; however, this is absent in the acute stage often making the diagnosis challenging especially overlapping with features of discitis/osteomyelitis. The majority of these lesions are asymptomatic; however, occasionally patients can present with pain. These are conservatively managed with symptomatic treatment.
References: Grivé E, Rovira A, Capellades J, et al. Radiologic findings in two cases of acute Schmörl’s nodes. AJNR Am J Neuroradiol 1999;20(9):1717-1721.
Wagner AL, Murtagh FR, Arrington JA, et al. Relationship of Schmorl’s nodes to vertebral body endplate fractures and acute endplate disk extrusions. AJNR Am J Neuroradiol 2000;21(2):276-281.
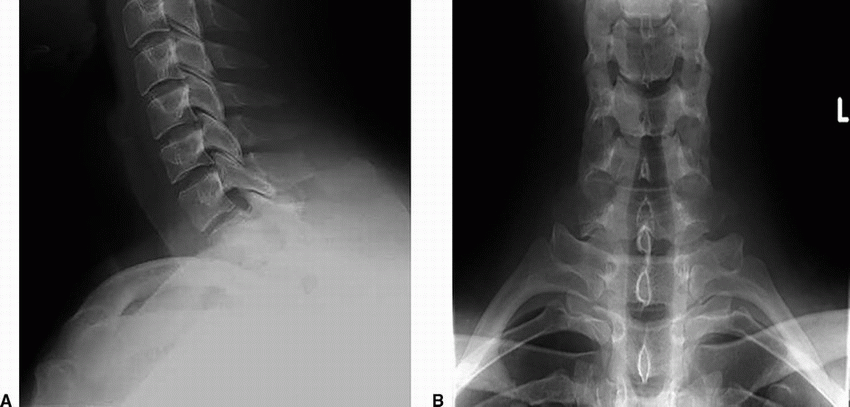
3 A 34-year-old male presents with pain in lower neck after a weight-lifting accident in the gym. There was focal tenderness on palpation in the lower cervical spine on examination. The patient was neurologically intact. A radiograph of the cervical spine was performed, provided below.
|
What is the most likely diagnosis?
A. Muscular strain with neck spasm
B. Possible facet fracture, CT is recommended.
C. Clay shoveler’s fracture
D. Normal study
View Answer
3 Answer C. Clay shoveler’s fracture. There is a fracture of C7 spinous process. The facets are intact.
|
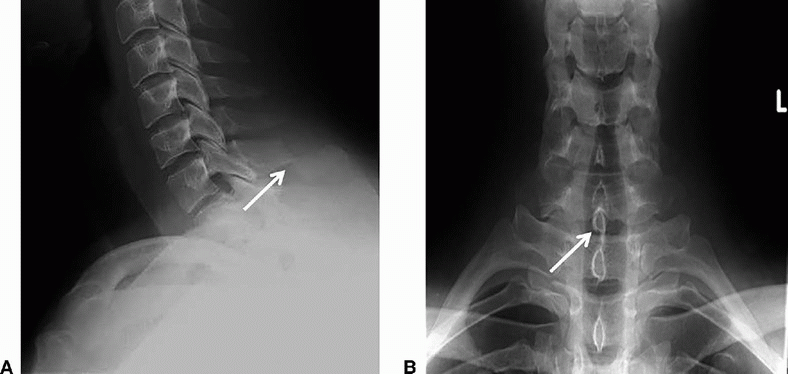
Imaging Findings: Lateral cervical radiograph: Oblique fracture of C7 spinous process. AP radiograph demonstrates double spinous process of C7 due to inferior displacement of fracture fragment.
Discussion: Clay shoveler’s fracture. This is an avulsion fracture of the spinous process, most commonly C7. It can result from both hyperflexion and hyperextension injury as well as direct trauma to the spinous processes. It is mostly seen on x-ray/CT as an oblique fracture of the spinous process midway between the tip and lamina with posterior-inferior displacement of distal fracture fragment. On frontal radiograph, displaced fracture fragment appears as double spinous process of the involved vertebra. Management is mostly conservative as this injury in isolation is neurologically stable.
Reference: Posthuma de Boer J, van Wulfften Palthe AF, Stadhouder A, et al. The Clay Shoveler’s fracture: a case report and review of the literature. J Emerg Med 2016;51(3):292-297.
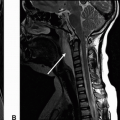
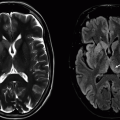
4 Key images from MRI performed for evaluation of back pain in the setting of fall are provided below.
|
4a What is the most likely diagnosis?
A. Osteomyelitis with epidural phlegmon/abscess
B. Metastatic disease
C. Compression fracture and epidural hematoma
D. Epidural lipomatosis
4b Which of the following is correct regarding the above entity?
A. Urgent neurosurgery consultation
B. Check inflammatory markers.
C. Get follow-up MRI in 6 weeks.
D. Obtain bone scan.
View Answer
4b Answer A. Urgent neurosurgery consultation.
|
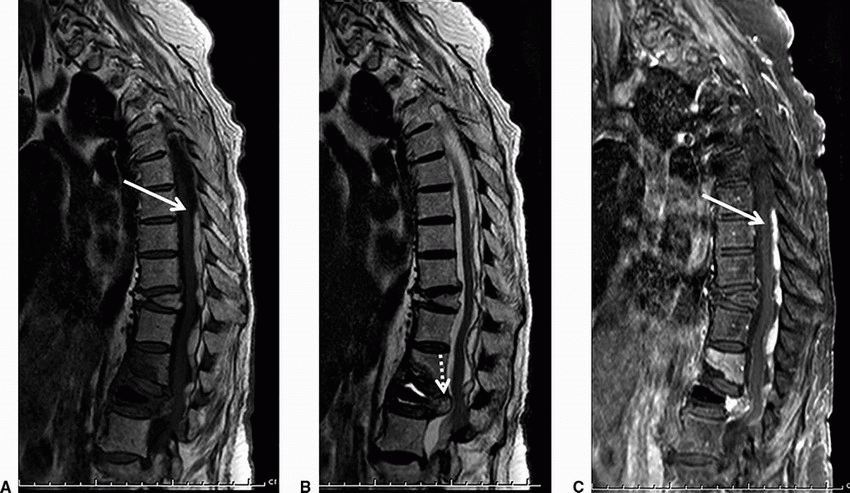
Imaging Findings: Sagittal T1, sagittal T2, and sagittal T1w fat-saturated postcontrast images demonstrate abnormal T1 and T2 hyperintense collection in the posterior epidural space (solid arrow A, B, and C). Note acute disc herniation (dotted arrow, B) with hemorrhage/edema within the herniated disc. Acute compression fracture of L2, postvertebroplasty changes in L3, and a chronic compression fracture of T12 are also seen.
Discussion: Spinal epidural hematoma. Hemorrhage in the spinal epidural space may be traumatic or nontraumatic in etiology. MRI is the most sensitive imaging modality for detection. MR signal depends on age of hemorrhage. Acute blood is isointense on T1 and hyperintense on T2w images, whereas in the subacute stage, methemoglobin results in T1 high signal as seen in the case above. Fat-saturated sequences differentiate it from epidural lipomatosis, and administration of gadolinium helps differentiate from enhancing epidural abnormalities including epidural phlegmon and neoplastic etiologies such as lymphoma and metastases.
Spinal epidural hematomas can result in devastating neurologic outcomes if unrecognized. Symptomatic patients often require urgent decompression to preserve neurologic function.
References: Al-Mutair A, Bednar DA. Spinal epidural hematoma. J Am Acad Orthop Surg 2010;18(8):494-502.
Braun P, et al. MRI findings in spinal subdural and epidural hematomas. Eur J Radiol 2007;64(1):119-125.
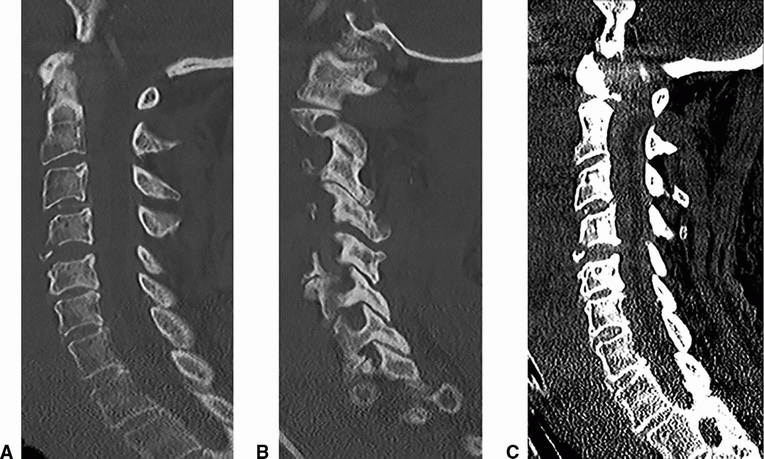
A. Flexion teardrop fracture
B. Extension teardrop fracture
C. Anterior disc ossification
D. Lytic endplate metastasis
View Answer
5 Answers A. Flexion teardrop fracture.
|
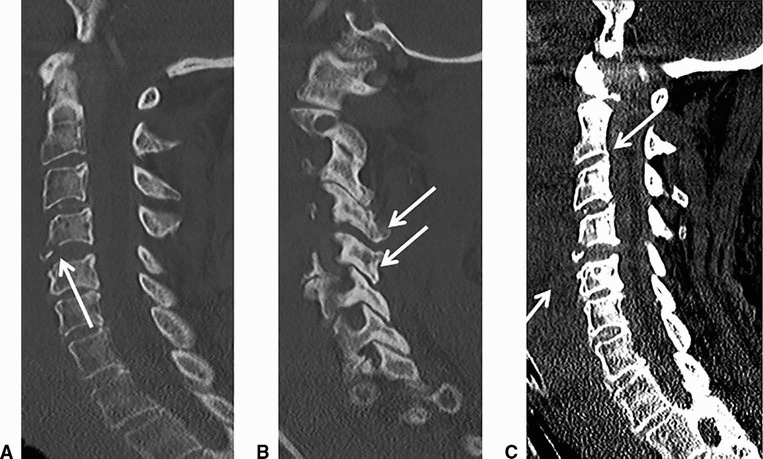
Imaging Findings: Multiple sagittal images of the cervical spine demonstrate a triangular bone fragment (solid arrow A) at the anteroinferior C4 vertebral body, along with widening of interspinous distance, widened facet joint (solid arrow B), as well as widened C4-C5 disc space suggestive of a three-column injury.
There is severe prevertebral soft tissue swelling (C). Also note the epidural hematoma spanning the entire cervical canal best seen on image C.
Discussion: Flexion teardrop fracture results from severe hyperflexion and axial compression injury of the cervical spine such as diving head first into a shallow pool. “Teardrop” refers to the triangular shape of the bone fragment at the anteroinferior (more common) or posteroinferior angle of the vertebral body typically C5/C6.
Hyperflexion injury results in disruption of the posterior ligaments with progressive injury resulting in posterior longitudinal ligament and discal disruption from posterior to anterior. Fracture of the anterior vertebral body completes the three-column injury.
These injuries are often associated with retropulsion of the posterior vertebral body fragment resulting in mass effect on the anterior spinal cord. Additional vertebral body and posterior element fractures are often seen.
It is important to recognize subtle signs of posterior ligamentous disruption on CT imaging especially in patients in a cervical collar. Look for widened interspinous distance, incongruity or widening of facet joints, and asymmetric widening of the disc in addition to osseous injuries. Lastly, attention should always be paid to the prevertebral and epidural soft tissues to detect any obvious hemorrhage such as in the case shown.
References: Bari D, Bernstein MP. Imaging of spine trauma. Semin Roentgenol 2016;51(3):180-202.
Kim KS, Chen HH, Russell EJ, et al. Flexion teardrop fracture of the cervical spine: radiographic characteristics. AJR Am J Roentgenol 1989;152(2):319-326.
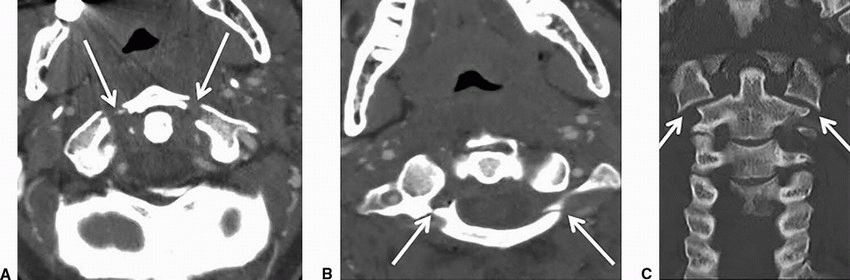
A. Bilateral C2 pars interarticularis fractures
B. C1 anterior ring fracture
C. Atlanto-occipital disassociation
D. Bilateral perched facets
View Answer
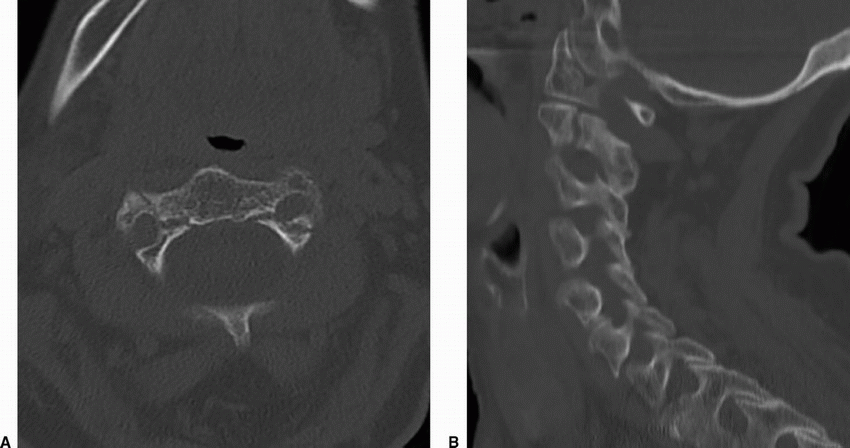
6a Answer A. Bilateral C2 pars interarticularis fractures. Bilateral C2 pars interarticularis fractures, often described as “hangman’s fracture.”
6b Which additional imaging investigation is warranted in this patient?
A. CT angiogram of the neck
B. CT angiogram of the head
C. MRI brain without contrast
D. CT neck soft tissues with contrast
View Answer
6b Answer A. CT angiogram of the neck. Extension through bilateral transverse foramen is seen, indicating need for CTA or MRA neck for assessment of potential vertebral artery injury.
|
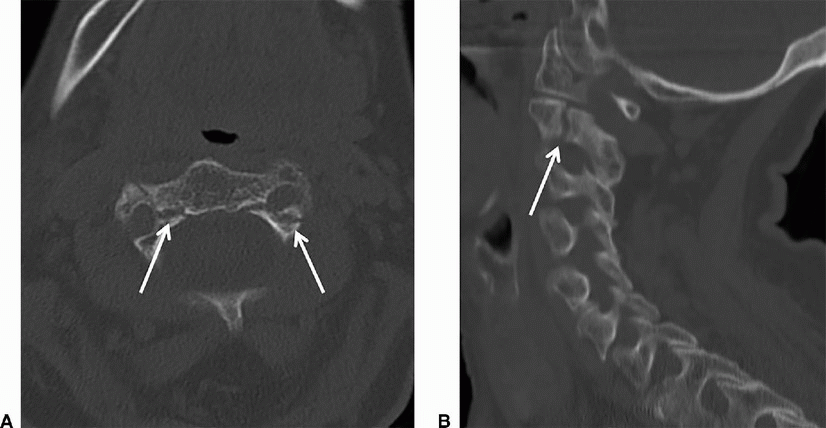
Imaging Findings: There is a linear fracture seen along bilateral C2 pars interarticularis (A and B). Note that the fracture margin extends into the transverse foramen. Therefore, a CTA or MRA neck to evaluate for potential vertebral artery injury is necessary (A).
Discussion: Hangman’s fracture or traumatic bilateral pars interarticularis fractures of C2. It is typically seen with hyperextension and distraction such as with hanging; however, it may result from both hyperflexion and hyperextension injury.
There are three types based on extent of translation and angulation (Effendi classification):
Type 1: Minimal translation (<2 mm, no angulation)
Type 2: Anterior translation with anterior angulation of more than 11 degrees
Type 2A: Severe angulation without anterior translation
Type 3: Bilateral fracture dislocation
Look for associated fractures of odontoid and C1. Although classically described as pars fractures, any part of the C2 ring including posterior vertebral body, pedicles, and laminae may be involved.
References: Dane B, Bernstein MP. Imaging of spine trauma. Semin Roentgenol 2016;51(3):180-202.
David D, Letzing M, Sliker CW, et al. Multidetector CT of blunt cervical spine trauma in adults. Radiographics 2014;34(7):1842-1865.
7 A 27-year-old male with motor vehicle accident, key images are shown below.
|
7a What is the most common mechanism of injury to cause the fracture shown?
A. Hyperextension
B. Hyperflexion
C. Rotation
D. Axial loading
7b Which of the following C1 fractures is considered most unstable?
A. Isolated anterior arch fracture
B. Isolated posterior arch fracture
C. Burst fracture with intact transverse ligament
D. Burst fracture with disruption of transverse ligament
View Answer
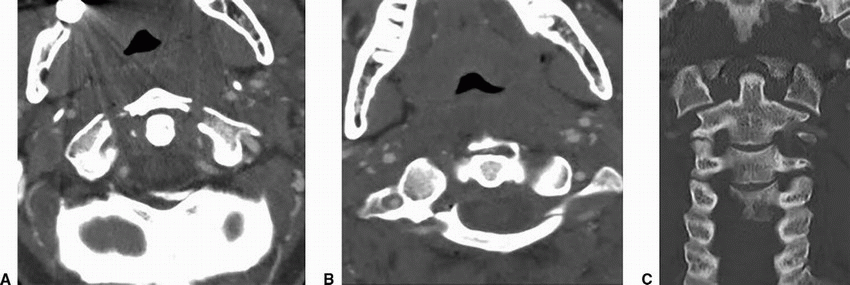
7b Answer D. Burst fracture with disruption of transverse ligament.
|
Imaging Findings: Images A and B show fractures through anterior and posterior arch of C1. Coronal image through the cervical spine demonstrates offset of the lateral masses of C1 and C2.
Discussion: Jefferson fracture. Burst fracture of C1 (Atlas) resulting from axial loading injury. C1 is a ring-shaped vertebra that comprises anterior arch, posterior arch, and two lateral masses, which articulate superiorly with occipital condyles and inferiorly with lateral masses of C2. The classic Jefferson fracture is a 4-part fracture with four fractures, two involving junction of anterior arch with the lateral masses and two fractures at the junction of posterior arch and lateral masses. Isolated arch fractures or lateral mass fractures may also occur.
Most patients remain neurologically intact. Clinical management often depends on integrity of the transverse atlantal ligament, which is instrumental in preserving atlantoaxial stability. This can be assessed directly with MRI. On open mouth view radiographs or coronal CT, sum of lateral displacement of lateral masses of C1 over C2 exceeding 7 mm is considered as a sign of transverse ligament injury (rule of Spence).
Congenital fusion anomalies of the anterior or posterior arch may mimic fractures but can be differentiated by their well-corticated edges.
References: Dane B, Bernstein MP. Imaging of spine trauma. Semin Roentgenol 2016;51(3):180-202.
Dreizin D, Letzing M, Sliker CW, et al. Multidetector CT of blunt cervical spine trauma in adults. Radiographics 2014;34(7):1842-1865.

A. Os odontoideum
B. Type 1 odontoid fracture
C. Type 2 odontoid fracture
D. Type 3 odontoid fracture
View Answer
8 Answer C. Type 2 odontoid fracture. There is a fracture at the base of the dens without extension of the fracture line into the body of C2, compatible with a type 2 odontoid fracture.
|
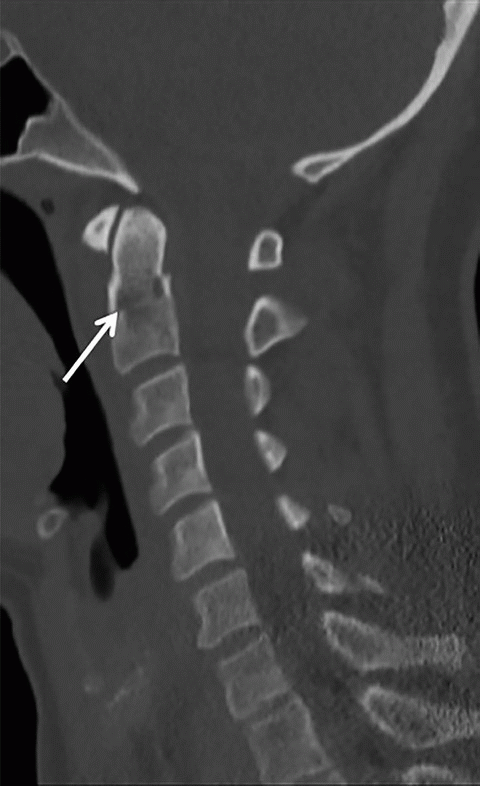
Imaging Findings: Top left sagittal CT image through the cervical spine demonstrates a nondisplaced fracture through the base of the odontoid process. Top right coronal CT image shows no extension of the fracture line into the body of C2, compatible with type 2 odontoid fracture.
Discussion: Odontoid fracture is the most common fracture of C2. They may result from hyperflexion or hyperextension injuries. It is common in the elderly even with low-energy trauma.
Types of odontoid fracture:
Type 1: Avulsion fracture of the alar ligament involving the tip of odontoid
Type 2: Fracture through base of dens; usually unstable
Type 3: Fracture through base of dens with extension into body of C2
Differential Diagnosis: It is important to differentiate odontoid fractures from common variants at this location.
Os odontoideum: Well-corticated ossicle in association with a hypoplastic odontoid process, often accompanied by hypertrophy of C1 anterior arch.
Ossiculum terminale: Small well-corticated bone just superior to the odontoid tip with a normal-appearing den.
References: Dreizin D, Letzing M, Sliker CW, et al. Multidetector CT of blunt cervical spine trauma in adults. Radiographics 2014;34(7):1842-1865.
Munera F, Rivas LA, Nunez DB Jr, et al. Imaging evaluation of adult spinal injuries: emphasis on multidetector CT in cervical spine trauma. Radiology 2012;263(3):645-660.
9 A 75-year-old postmenopausal women with severe lower back pain had an MRI evaluation. Key images are shown below.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


