Authors
Treatment
Mean tumor size (cm)
Follow up (months)
No of patients
Cancer specific survival (%)
Local failure rate (%)
Lane et al. (2007) [6]
Partial nephrectomy
2.9
68
58
100
2.70
Barbalias et al. (1999) [3]
Partial nephrectomy
3.5
68
41
97.50
7.30
Radical nephrectomy
3.8
68
48
98.40
0
Butler et al. (1995) [2]
Partial nephrectomy
2.5
68
46
100
2.10
Radical nephrectomy
2.8
68
42
97
2.30
Liebovich et al. (2004) [4]
Partial nephrectomy
4.9
68
91
98
?
Radical nephrectomy
5.4
68
841
86
?
Nephron-sparing approaches have also shown potential to reduce the post surgical progression to significant chronic kidney disease requiring dialysis [5]. Huang et al., conducted a retrospective study of 662 patients with a normal serum creatinine undergoing elective partial or radical nephrectomy for small solitary renal tumors. Using estimated GFR and defining chronic kidney disease as a GFR <60 they found that the 3 year probability of CKD was 20 % in the partial nephrectomy group and 65 % in the radical nephrectomy group (p < 0.0001). A similar study conducted by La Rochelle et al., followed 84 patients undergoing partial nephrectomy and found the estimated 5 year end stage renal disease free survival in patients without local recurrence was 97 % at 5 years [7]. Hence, nephron-sparing approaches can preserve renal function without compromising local control or survival. Laparoscopic partial nephrectomy (LPN) offers patients the same advantages over OPN as LRN but it is technically challenging surgery, which requires advanced laparoscopic skills [8]. In expert hands, LPN appears to offer excellent outcome for tumors <4 cm.
12.2.2 Non-surgical Nephron Sparing Approaches
Not all patients with renal cell carcinoma are suitable surgical candidates, and many patients due to medical comorbidities or body habitus are unable to undergo a nephrectomy. For these patients, other treatments have been used including cryoablation and radiofrequency ablation. These modalities have shown good cancer control outcomes in multiple published series. A meta-analysis of 47 studies in which patients underwent either RFA (775 cases) or cryoablation (600 cases) has recently been published [9]. There was no significant difference in mean patient age, tumor size or duration of follow-up. However, a greater number of the cryoablation patients underwent pretreatment biopsy and surgery via the laparoscopic route. The main findings were a local progression rate that was significantly higher after RFA than cryoablation (12.9 % vs. 5.2 %), and a greater need for repeat ablation with RFA than cryoablation (8.5 % vs. 1.3 %). Although metastasis was seen more commonly after RFA, the difference did not reach statistical significance in this meta-analysis. Lucas et al., retrospectively evaluated 242 patients undergoing radiofrequency ablation, partial nephrectomy or radical nephrectomy for unilateral renal masses smaller than 4 cm [10]. They reported the 3-year freedom from stage III chronic kidney disease for radio frequency ablation, partial nephrectomy and radical nephrectomy was 95.2, 70.7 and 39.9 %, respectively (p < 0.001)1. These results reaffirm that partial nephrectomy may better preserve renal function compared to radical nephrectomy, and also show that ablative therapies (which treat the tumor without removing the entire kidney) may also be effective for preserving renal function.
12.3 Radiation Therapy for Renal Cell Carcinoma
Conventional radiation therapy, used for almost all cancers, has not been routinely used for primary renal cell carcinoma as there has been no consistent survival benefit shown for either preoperative or postoperative radiation [11–14]. Juusela et al. randomized 88 patients to preoperative radiation therapy with 33 Gy over 3 weeks or immediate nephrectomy. Five year actuarial survival was 47 % in the radiation group and 63 % in the nephrectomy only group with no statistically significant difference [11]. Kjaer et al. conducted a prospective randomized trial comparing post nephrectomy radiation with 50 Gy in 20 fractions to observation and reported no significant difference in relapse rate or overall survival between the two groups [12]. Of the patients receiving radiation therapy in the later study 44 % reported serious GI side effects. As a result of these studies renal cell carcinoma has typically been thought of as “radioresistant” as it does not respond to conventional external beam radiation at the maximal dose that can be safely delivered.
A retrospective study by Wersall et al., looked at radiosurgical outcomes from 58 patients with extra cranial metastatic renal cell carcinoma or inoperable primary renal cancers. They were able to demonstrate radiologic regression in 30 % of patients, but more importantly a 90 % local control rate [13]. Based on these promising retrospective findings Svedman et al., conducted a prospective phase II trial treating a total of 82 extracranial renal cell carcinoma lesions (primary or metastatic). They were able to obtain local control, defined as radiologically stable disease or partial/complete response in 98 % of treated lesions [15]. These studies showed very encouraging results for the use of stereotactic radiosurgery to treat renal cell carcinoma.
12.4 Stereotactic Body Radiotherapy for Renal Cell Carcinoma
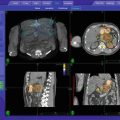
Preclinical and early clinical experience using radiosurgery to treat primary renal cancers appear promising as well: Ponsky et al., from the Cleveland Clinic have treated kidneys in ten female swine all with approximately 2 cm sized lesions with single fractions of 24–40 Gy using the CyberKnife [16]. Sixteen kidneys were harvested at 4, 6, or 8 weeks after treatment and pathologically examined. After 8 weeks, the kidney tumors were completely ablated with fibrosis with a zone of adjacent partial fibrosis. The renal parenchyma surrounding the area of partial fibrosis was histologically normal. Beitler et al. [17], from Staten Island University Hospital treated nine patients who refused surgery for clinically and radiographically non-metastatic renal cell carcinoma with 40 Gy in 5 fractions using conformal external radiation. At 2 years follow up none of the patients had recurred in the radiated area. Four of the nine patients were still alive with minimum follow up of 48 months.
Ponsky et al. [18], from the Cleveland Clinic treated three patients with radiologic evidence of renal tumor less than 4 cm with a total of 16 Gy in 4 fractions over 2 days using the CyberKnife as the first level of a dose escalation study. Patients then underwent partial or total nephrectomy 8 weeks after completion of radiosurgery and surgical specimens were reviewed histologically. All three patients’ tumors remained stable or reduced in size and one patient’s tumor was completely ablated. In these initial patients, no acute toxicities, no change in renal function and no change in clinical performance status were noted.
Related posts:
 Stereotactic Body Radiotherapy for Oligometastasis
Stereotactic Body Radiotherapy for Bone and Soft Tissue Sarcoma
Stereotactic Body Radiotherapy for Oligometastasis
Stereotactic Body Radiotherapy for Bone and Soft Tissue Sarcoma
 Stereotactic Body Radiotherapy (SBRT) for Pancreatic Cancer
Stereotactic Body Radiotherapy (SBRT) for Pancreatic Cancer
 Stereotactic Body Radiation Therapy to Liver
Stereotactic Body Radiation Therapy to Liver
 Stereotactic Body Radiotherapy in Head and Neck Cancer
Stereotactic Body Radiotherapy in Head and Neck Cancer
 Stereotactic Body Radiotherapy: A Practical Guide for the Delivery of Accelerated Partial Breast Irradiation
Stereotactic Body Radiotherapy: A Practical Guide for the Delivery of Accelerated Partial Breast Irradiation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


