Strain Elastography
3.1 Overview
Strain elasticity imaging (SE) determines the strain or elasticity of tissue. This corresponds to the stiffness or softness of a lesion; the higher the strain, the softer the lesion. To determine the strain of a tissue or lesion one must evaluate how the lesion deforms when an external force is applied. Each vendor has a different requirement for the optimal external force. This force can vary from minimal or no movement to moderate rhythmic force generated by probe movement. Therefore the technique for obtaining a good strain elastogram varies depending on the vendor.
3.2 Technique/How to Perform an Examination
The technique of measuring how a lesion changes when an external force is applied is strain elastography (SE), one type of elasticity imaging as discussed in Chapter ▶ 2. If patient movement such as breathing, heartbeat, or external compression with rhythmic motion of the ultrasound transducer is used as the source of the movement, this technique is called SE using the manual compression method. In SE the absolute strain value (stiffness) cannot be calculated because the amount of the push cannot be accurately measured. The real-time elasticity image is displayed with a scale based on the relative strain of the tissues in the image displays strain distribution, indicating relative stiffness as a two-dimensional (2D) overlay. The clinical implications of this are discussed in detail in the interpretation section later in this chapter.
One can also use a low-frequency ultrasound pulse (a push pulse) as the source of the displacement. This technique is called acoustic radiation force impulse (ARFI) (see Chapter ▶ 2).21 A strain image can be obtained by using ARFI and analyzing the displacement changes with a similar strain algorithm. Note that this is different from shear wave elastography (SWE), where the velocities of the shear waves generated as a result of the push pulse are measured.
Strain EI of the breast is performed with a conventional ultrasound unit and a standard ultrasound breast transducer. Specific software analysis of frame-to-frame difference in deformation in tissue with mild compression allows for the display of the “softness” or “stiffness” of a lesion.
The technique required to obtain the optimal images varies with the type of SE being used as well as the manufacturer of the system. For SE the amount of external displacement (compression/release cycle) needed varies depending on the algorithm used. With some manufacturers very little if any manual compression/release is needed, whereas with others a rhythmic compression/release cycle is required. With experience and practice one can optimize the compression used to obtain optimal image quality.
The algorithm used in compression elastography requires that the strain changes remain within the imaging plane. The same slice of the lesion needs to remain in the imaging plane during the compression/release cycle (▶ Fig. 3.1). Optimal images can be obtained by monitoring the B-mode image to confirm the lesion is displaced only in depth during scanning and is otherwise not moving in the field of view (FOV). To avoid having the lesion move in and out of plane we prefer to position the patient so that an imaginary line through the transducer face and lesion is perpendicular to the floor with the patient’s breathing moving the lesion in the same plane (▶ Fig. 3.2a,b). The transducer should not be angled either superiorly or inferiorly (▶ Fig. 3.2c) nor to the right or the left (▶ Fig. 3.2d).
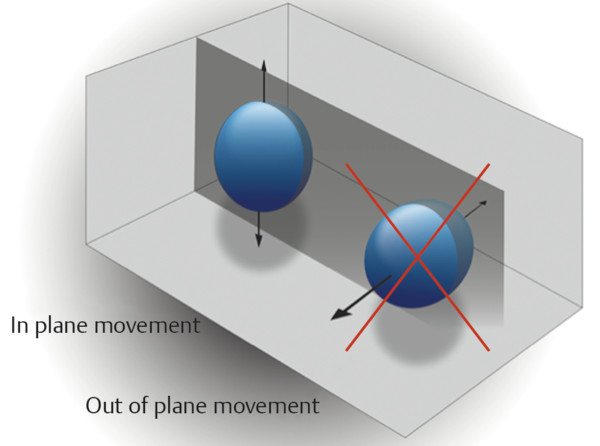
Fig. 3.1 When performing strain elastography it is important that the same image plane through a lesion be maintained during data acquisition. The gray plane corresponds to the ultrasound beam. An optimal elastogram is obtained with in-plane movement of the lesion. Out-of-plane movement may result in inaccurate elastography results.
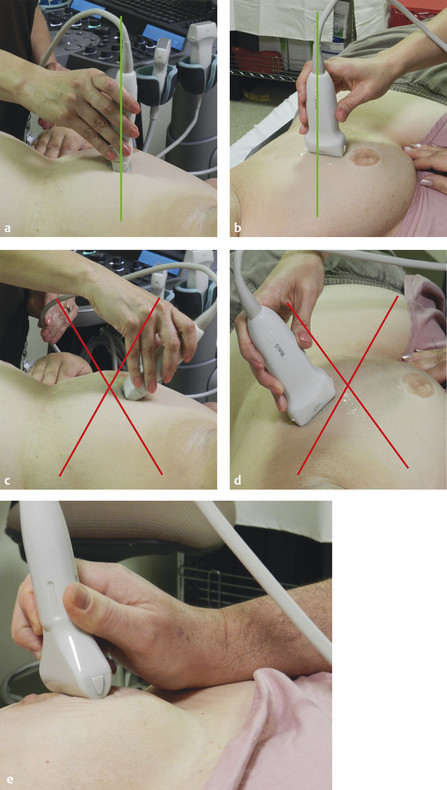
Fig. 3.2 Patient and transducer positioning is important in obtaining optimal elastograms. The patient should be positioned so that the imaging plane is in the same plane as the patient’s respiration movements. Proper positioning is demonstrated in (a) and (b). Positioning the transducer as in (c) and (d) is not recommended. Placing the wrist of the scanning hand on the patient will help stabilize the transducer and improve the ability to apply fine movements (e).
The lesion should appear similar on all frames of the SE clip. If not, there is too much displacement of the lesion during scanning or unacceptable precompression is being applied. With SE one cannot survey the breast; scanning must be done in one stationary position.
Most systems use a dual display; one with the B-mode image and the other with the elastographic data. The elastographic data can be superimposed over a B-mode image. In this case the B-mode image is usually displayed in gray scale and the elastogram in a color scale (▶ Fig. 3.3a). We choose to use a gray scale map for image depiction with white as soft and black as hard (▶ Fig. 3.3b). In this situation we do not display the B-mode image superimposed on the elastogram. The use of two gray scale maps interferes with interpretation. We use a gray scale in SE because we believe we can identify the changes in relative stiffness more accurately than with use of a color scale, where a small change in relative stiffness may be depicted as an abrupt color change. We also believe we are able to measure a lesion more accurately on the elastogram using the gray scale. Color maps can be used; preference is often determined by the user’s exposure to elastography and interpretation. If color maps are used be careful to document which scale you are using because some have red as stiff and others blue as stiff. The color scale should always be included with the image for accurate interpretation. Because of the relative scale in SE we do not find color useful. However, in SWE, where an absolute value of stiffness is obtained, color coding can be very useful in interpretation.
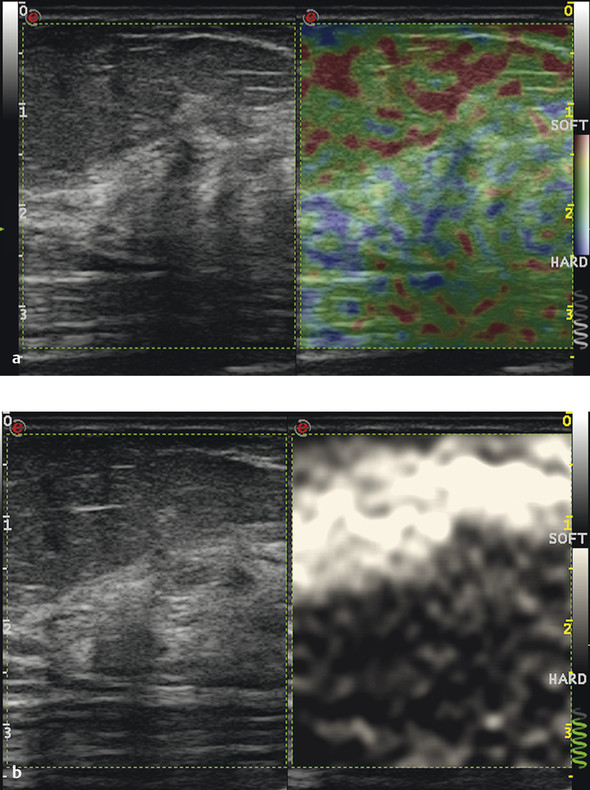
Fig. 3.3 The strain elastography appearance of normal glandular tissue and fat is presented using the color scale with blue as stiff (a) and with the gray scale map (b). Note that the image contains fat, glandular tissue, and the pectoralis muscle.
3.2.1 Performing an Examination
SE images are generated from the raw data of B-mode images. Therefore it is important to obtain quality B-mode images before activating the strain mode. It is important to maintain the transducer perpendicular to the skin (▶ Fig. 3.2). Find a scanning window that allows for stable positioning of the transducer with the compression/release cycle.23 Placing the wrist of the hand on the patient helps stabilize the transducer and allows for more sensitive movements (▶ Fig. 3.2e).
You must use the appropriate amount of compression/release cycle for the system you are using. The presently available systems use one of three types of compression/release: no manual compression, minimal compression or vibration, and moderate compression. The amount of compression may vary with the size of the breast or the depth of the lesion. With experience and practice one can learn the optimal compression/release needed for an optimal quality elastogram for a given system.18 The B-mode image is useful to access the amount of tissue displacement. ▶ Table 3.1 lists the various available systems and the techniques they require.
| Technique | Product name | Vendor |
| No manual compression | eSie Touch | Siemens (Mountain View, CA) |
| Elastography | Philips (Bothell, WA) | |
| Minimal compression | ElaXto | Esaote (Indianapolis, IN) |
| Real-time tissue elastography (RTE) | Hitachi Aloka (Wallingford, CT) | |
| Elastography | Toshiba (Minato, Tokyo, Japan) | |
| Moderate compression | Elastography | GE (Fairfield, CT) |
| Real-time tissue elastography (RTE) | Hitachi Aloka (Wallingford, CT) | |
| Elastography | Zonare/Mindray (Shenzhen, China) |
3.2.1.1 No Manual Compression Systems
Place the probe vertically on the skin without consciously applying any vibration/compression (▶ Fig. 3.2). Keep the probe lightly touching the skin and try not to apply pressure. It is important to keep the transducer perpendicular with no pressure (minimal precompression) and without movement on the skin above a target. A technique to consistently apply minimal precompression has been described19 and is discussed in detail in Chapter ▶ 3.2.3.
This method gets the compression/decompression cycle from vibration caused by involuntary muscle contraction in the hand and vibration caused by muscle contraction, breathing, and heartbeat of the patient. There is minimal tissue movement, so extremely fine image display is possible. However, in some cases with large breasts or deep lesions minimal compression/release movement with the transducer or transducer vibration may be required to obtain the optimal elastogram. In patients with small breasts the motion may still be too great and having the patient hold her breath may be helpful in obtaining optimal elastograms.
3.2.1.2 Minimal Compression/Vibration Systems
Place the probe vertically on the skin and apply very mild vibration (compression/release cycle). Ensure that you do not push too hard. The compression/release stroke should be no more than 1 mm. Keep the probe lightly touching the skin, and apply extremely fine vibration with a fast cycle, as if lifting up the skin with the probe. This method can be used for relatively shallow lesions to moderately deep lesions, and it allows elastography imaging of fine targets several millimeters in size such as nonmass abnormalities. It is also possible to depict in detail the distribution of soft areas (areas with significant strain), and it provides a great deal of diagnostic information.23 The frequency and degree of displacement of the compression/release cycle can be varied to identify the optimal technique. For learning the technique it is recommended that the scanner vary the degree of compression/release cycle as well as the frequency of the compression/release cycle and observe the changes in the elastogram. With the appropriate technique there should be minimal changes in the appearance of the elastogram.
3.2.1.3 Moderate Displacement Systems
Place the probe vertically on the skin, and apply fairly moderate compression/release (about 1–2 mm) similar to the minimal displacement technique except for applying more probe displacement. This method was recommended on older systems, but some newer systems now require much less motion. On the systems that require no displacement, the use of this moderate displacement technique will generate an elastogram composed of noise. This technique requires more skill to avoid precompression and thereby maintain scanning in the same location of the lesion (out-of-plane movement of the lesion).
3.2.2 Degree of Displacement Measuring Tools
Some devices have a display bar or number to confirm that you are applying the appropriate amount of displacement (compression/release cycle) to generate the elastogram (▶ Fig. 3.4). When the appropriate amount of displacement is being applied, the number display or the color bar has the maximum value. If the displacement is either too great or too small the number display or color bar shows a lower value. When learning how to perform SE with the manual displacement method, it is helpful to practice varying the amount of displacement and frequency of displacement while watching the display bar or number. You can identify the appropriate technique required by experimenting with your displacement technique and using the color bar or number to identify the optimal technique for your system. When the appropriate technique is used the elastogram should be similar on all frames. Some systems provide a visual scale on the frequency and amount of displacement you are generating. This real-time feedback bar or number only evaluates the amount of lesion displacement (tissue deformation). Other factors are important in obtaining optimal images so a high quality factor does not guarantee you will have optimal images.
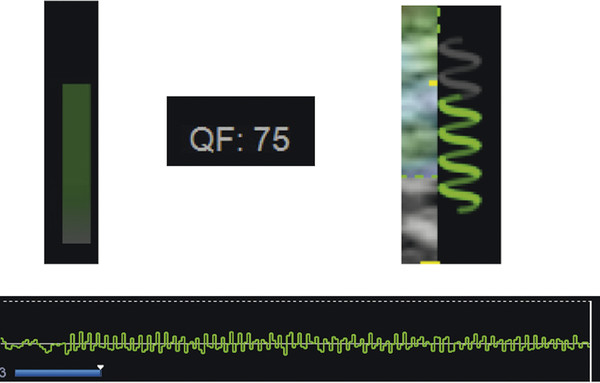
Fig. 3.4 Various numerical or visual scales are used to optimize the amount of the compression/release cycle. Several of them are presented in this image. When the appropriate amount of compression/release is applied the scales are maximized. If the compression/release cycle is either too great or too small the scale will be minimized.
3.2.3 Precompression
A critical factor in generating a diagnostic elastogram is the amount of pressure you apply when scanning. This is called precompression (▶ Fig. 3.5). This is different than the amount of displacement (compression/release) you are applying. If you scan with a “heavy hand” you compress the tissues and change their elastic properties. For example, if you have a balloon filled with air and lightly touch the balloon you create a moderate displacement of the balloon. However, if you compress the balloon between two heavy books and use the same amount of pressure you will create a much smaller displacement because the compression caused by the books increases the air pressure in the balloon. This precompression markedly changes the image quality and can significantly affect results (see ▶ Fig. 2.4). This is confirmed with shear wave technology where the shear wave velocity can change by a factor of 10 based on precompression (▶ Fig. 3.6). In ▶ Fig. 2.5 graphs the effects of precompression for various tissues that occur in the breast. Note that as precompression increases the differences in shear wave velocity between tissue types decrease, leading to less conspicuity between tissues. If enough precompression is applied all tissues are similar, and the elastogram changes are mostly noise. Chapter ▶ 2 provides a detailed discussion of the effects of precompression on both SE and SWE.
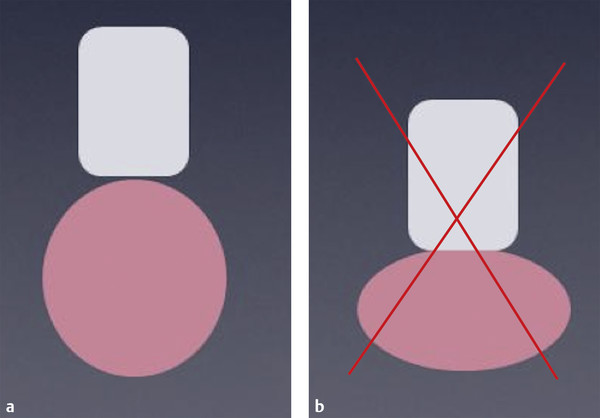
Fig. 3.5 Precompression should not be applied to the breast when obtaining an elastogram. (a) Minimal precompression applied to the breast. (b) Precompression applied to the breast. Note the dimpling of the breast caused by the pressure of the transducer.
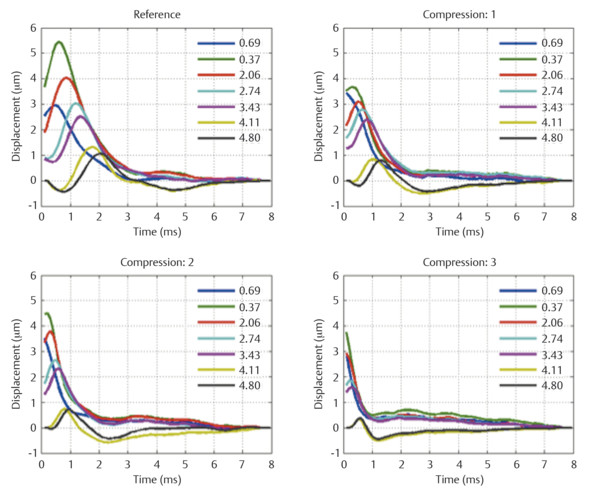
Fig. 3.6 The effect on shear waves speed with the application of precompression on normal breast tissue is shown in this figure. The graphs display the tissue displacement at various locations from the acoustic radiation force impulse (ARFI) pulse over time. The reference image was obtained with minimal precompression, whereas the other graphs were obtained with increasing amounts of precompression. Note that as precompression is applied the tissue displacement occurs sooner (increased shear wave velocity).
(Reprinted with permission from Barr RG, Zhang Z. Effects of precompression on elasticity imaging of the breast: development of a clinically useful semiquantitative method of precompression assessment. J Ultrasound Med 2012;31(6):895–902)
The following technique has been suggested to apply only a minimal amount of precompression reproducibly.19 In general some amount of precompression is applied to obtain the B-mode image because it improves B-mode image quality (▶ Fig. 3.7). When obtaining the elastogram focus on an object in the FOV (e.g., a rib). Lift the transducer, watching the object in B-mode. As the transducer is lifted (decreasing the precompression) the object moves deeper in the image. When the object is as deep in the image as possible and adequate probe contact is maintained, the elastogram is obtained. This technique has been shown to be highly reproducible both intraoperator and interoperator.19 This is a similar technique used for color Doppler imaging because precompression can occlude blood vessels. The use of a large amount of coupling gel is helpful. The “quality factor” or “compression bar” used in some manufacturers’ equipment does not assess the amount of precompression being applied.
Better-quality elastograms can be obtained if the patient raises the ipsilateral hand above the head, the patient is positioned so the transducer is perpendicular to the floor (▶ Fig. 3.2), lesion motion with respiration moves the lesion within the imaging plane, and the patient refrains from talking during data acquisition.
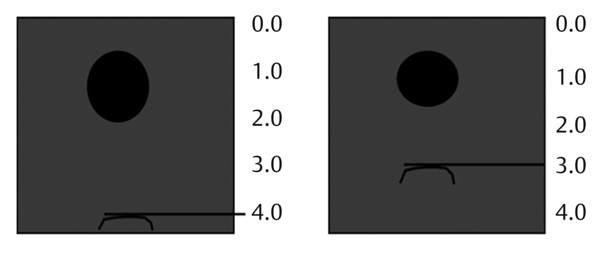
Fig. 3.7 A technique to confirm that minimal precompression is applied has been proposed. A structure in the far field of the image is identified (i.e., rib or Cooper ligament). As the transducer is lifted the structure will move deeper in the image. When the structure is as deep in the far field as possible and adequate contact with the transducer is maintained minimal precompression is applied and an optimal elastogram will be obtained. In this pictogram the rib with minimal precompression was located at 4 cm depth. If precompression is applied such that the rib is at 3 cm depth this would be considered a 25% precompression.
(Reprinted with permission from Barr RG, Zhang Z. Effects of precompression on elasticity imaging of the breast: development of a clinically useful semiquantitative method of precompression assessment. J Ultrasound Med 2012;31(6):895–902)
The center of the lesion does not have to be used to obtain the elastogram. In fact it is better if a lesion position is chosen where the lesion measures between 1 and 1.5 cm. This allows for other tissues to be included in the FOV and accounts for size changes that occur in cancers in elastography. A malignant lesion may appear more than three times the size of the B-mode image. Therefore, if you have a 2 cm malignancy on B-mode it may appear as 6 cm on the elastogram, filling the entire FOV, and may not be appreciated. The size changes are discussed in detail in the interpretation section of this chapter.
Results can be displayed in gray scale or with various color displays; preference is often determined by the user’s exposure to elastography and preference in interpretation. If a color map is used care must be taken because a standard has not been established, and a color map using red as stiff or the opposite color map with blue as stiff can be used. The color scale should always be included on the image for accurate interpretation. It is important to remember that in SE a relative scale is displayed and should not be confused with SWE where an absolute stiffness value is obtained and color coded on a per pixel basis. In SWE, all vendors use the standard of red as stiff and blue as soft. Remember SE is a relative technique, and a lesion may appear a different shade of gray or color depending on the other tissues in the FOV (see ▶ Fig. 2.2). For example, in a patient with normal glandular breast tissue and fat, the fat will appear soft because it is the softest tissue in the FOV. However, if only fat is in the FOV, some of the fat will appear hard because it is the hardest tissue in the FOV (see ▶ Fig. 2.3). This can cause difficulty in interpretation. By including some fat, normal dense breast tissue, pectoralis muscle, and the lesion in the elastogram FOV, one can minimize these changes between images. This is discussed in detail in Chapter ▶ 2. Having a soft tissue (fat) and a harder tissue (muscle) helps maintain a similar gray scale or color display (dynamic range of mapping). A large FOV is helpful in image interpretation because including more tissue will set a scale that allows for better differentiation between tissues.
If an ARFI push pulse is used to generate the tissue displacement (Virtual Touch Imaging [VTI], Siemens Ultrasound, Mountain View, CA), then no manual displacement should be used. The probe should be held steady, and the patient should remain motionless, with no breathing or talking during the acquisition. Because of the acoustic power of the ARFI pulse, the system will freeze for a few seconds for transducer cooling. During this period the system will not respond to knob activation. The algorithm used to generate the elastogram is similar to that for SE on the same system. In general the ARFI push pulse is limited in producing displacement deeper than 4 to 5 cm with the breast imaging transducer. If the lesion is deeper a satisfactory elastogram may not be obtained. The image displays are similar to those for SE images with the B-mode image on the left and the VTI elastogram on the right. When using an ARFI pulse to generate a strain image a region of interest (ROI) box is placed at the site of the lesion. The ARFI pulse is generated only within the ROI box, therefore only the ROI box has strain data within it on the elastogram (▶ Fig. 3.8).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


