SUBMANDIBULAR GLAND AND SPACE DEVELOPMENTAL ANOMALIES
KEY POINTS
- Imaging is central to a proper diagnosis of submandibular and submental space anomalies.
- Computed tomography and magnetic resonance are the prime diagnostic imaging tools.
- Ultrasound is cost additive, not definitive, and should be avoided in almost all cases for these reasons.
Developmental abnormalities involving the submandibular and submental region are mainly those due to epidermoid and dermoid cysts and venolymphatic malformations (Figs. 180.1–180.5). Branchial apparatus anomalies and those of thyroglossal duct migration origin occasionally enter the differential list under the category of developmental conditions before imaging is completed (Fig. 180.6). These anomalies are almost never syndromic or associated with craniofacial anomalies. A ranula will often transiently enter the differential picture because of its cystic nature (Fig. 180.4).
Proliferative hemangiomas and venolymphatic malformations may originate in the submandibular space or gland, spread transcompartmentally, or be isolated to the space and/or gland (Fig. 180.5).
ANATOMIC AND DEVELOPMENTAL CONSIDERATIONS
Embryology
The developmental background related to proliferative hemangiomas and vascular malformations and their classifications is discussed in Chapter 9, while that of epidermoid and dermoid cysts and teratomas is discussed in Chapter 8 and the thyroglossal duct in Chapter 170.
IMAGING APPROACH
Techniques and Relevant Aspects
These anomalies are generally evaluated by computed tomography (CT) and magnetic resonance imaging (MRI) as described in Chapter 175 for major salivary gland region masses. Detailed mandibular reconstructions may occasionally need to be part of the CT protocol. Contrast should be used in almost all cases.
Pros and Cons
CT is generally more suitable as a starting point in anomalies that present as a submandibular or submental space region mass, either bland or inflammatory; its only drawback is the use of ionizing radiation. MRI may be used initially but will require general anesthesia in many young children. Ultrasound is cost additive and not definitive for the entirety of medical decision making required in the overwhelming majority of cases since all it usually does is confirm the cystic nature of the mass and cannot provide definitive information about sometimes important associated findings if it is an anomaly or associated findings that might lead to a different diagnostic consideration.
If a venolymphatic malformation is the primary working diagnosis, then MRI is the preferable primary imaging tool (Fig. 180.5).
MANIFESTATIONS AND FINDINGS
Computed Tomography, Magnetic Resonance Imaging, and Ultrasound
The general appearance of simple, infected, and otherwise complicated cysts is described in Chapters 8 and 13. The pathoanatomic relationships of these cysts findings are variable. The cysts typically are located in the submandibular and/or submental space, outside of and displacing the gland (Figs. 180.1–180.4). The cysts may also track to the floor of the mouth, parapharyngeal space, and upper deep neck spaces. A defect in the mylohyoid muscle, for the passage of a neurovascular bundle and accessory salivary tissue, or the open back edge of the mylohyoid provides potential access to the floor of the mouth and, in particular, the sublingual space (Figs. 180.1–180.3).
The appearance of epidermoid and dermoid cysts and teratomas is discussed in Chapter 8 (Figs. 180.1–180.3 and 180.7).
The appearance of venolymphatic malformations is discussed in Chapter 9 (Fig. 180.5).
The morphologic variations of thyroglossal duct development that may result in masses in or adjacent to the submandibular space is discussed in Chapter 170 (Fig. 180.6).
DIFFERENTIAL DIAGNOSIS
From Clinical Data
A history of intermittent changes in size or inflammation will suggest a branchial apparatus or possibly thyroglossal duct cyst as a possible etiology, especially in children and young adults. Such characteristics can also suggest a venolymphatic malformation. Dermoid and epidermoid cysts will typically continuously and slowly enlarge. A bluish discoloration or change with Valsalva favors a malformation.
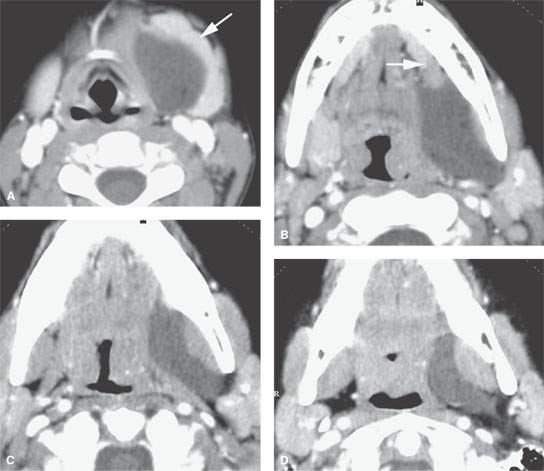
FIGURE 180.1. Contrast-enhanced computed tomography study in a patient presenting with a left submandibular region mass. In (A), a cyst displaces the submandibular gland (arrow). In (B), the cyst can be seen extending toward but barely entering the floor of the mouth over the back edge of the mylohyoid muscle (arrow). In (C), the cyst spreads out in the parapharyngeal space but respects the plane of the constrictor musculature of the pharynx and pterygomandibular raphe—a pattern that continues in (D); this pattern is a differentiating feature of this epidermoid cyst compared to a ranula.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Intraconal Orbit: Tumors
Intraconal Orbit: Tumors
 Hypopharynx: Developmental Abnormalities
Hypopharynx: Developmental Abnormalities
 Tumors of the Submandibular Gland and Space and Tumorlike Conditions
Tumors of the Submandibular Gland and Space and Tumorlike Conditions
 Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
Masticator Space, Buccal Space, and Infratemporal Fossa Infections and Other Inflammatory Conditions
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


