Renal transplants are a resource-heavy treatment modality. As the number of renal failure patients increase every year, so does the demand for donors. And despite the social media coverage and celebrity-driven organ donation campaigns, the rise in the number of donors does not keep pace with the rise in the number of new patients with renal failure who require renal replacement therapy, thereby putting additional stress on the dialysis centres and hospitals. Transplant gives patients a significant survival advantage. While the average survival of renal failure patients on haemodialysis is only 4 to 8 years, those who receive cadaveric transplants have a 5-year survival rate of 82%, and those who receive living donor kidneys have a 5-year survival rate of 90%. It therefore behoves the transplant team to make every donated kidney succeed. And a critical part of the recipe towards success in a renal transplant is the preoperative and postoperative assessment of the vascular status of both the donor and recipients; and early identification and timely management of postoperative complications. Since the first transplant in 1954, many refinements in diagnostic imaging for donor and recipient anatomy and surgical techniques in laparoscopic and robotic methods of donor organ harvest have taken place along with improvements in immunosuppressants and methods of organ matching. Donor criteria has been expanded in an effort to better utilize organs from extremes of age, borderline function and challenging anatomy. All these increase the technical challenges involved for each member of the transplant team.
Preoperative imaging of the donor
Donor imaging is only possible in live donors. Deceased (brain-dead) donors usually do not get imaging done. However, where possible it would help the transplant surgeon team to know the renal vasculature beforehand even in deceased donors. In modern times, where multiorgan harvest is becoming more and more common, knowing the donor’s renal vasculature preoperatively before the harvest will ensure that the team is aware of the presence of accessory renal vessels or anomalies. This would result in less incidence of injuries and therefore shorter warm ischaemia time. Also if there are less harvest-time injuries, it would decrease the time spent in bench dissection and repairing the injuries.
The most favourable anatomy that makes transplant easy is:
1. Single renal artery and vein
2. Long pedicle of renal artery and vein (ideally 3 cm for artery and 3 cm for vein)
3. Absence of plaque or stenosis in the donor artery
4. Absence of webs or trabeculations in the renal vein suggestive of renal vein thrombosis
Generally the left donor kidney satisfies the above anatomical conditions, and is therefore preferred
The various anomalies and pathologies and how they affect the surgical decisions:
1. Main renal artery orthogonal diameter – The kidney with the bigger renal artery orthogonal diameter may be preferred. Diameter <2 mm is a high risk of thrombosis and graft failure.
2. Accessory renal arteries – If two or more arteries each with a separate ostium from the aorta are supplying a kidney, then the one with the largest diameter is called the main renal artery and the others are called accessory arteries. For each accessory artery, it is important to measure the orthogonal diameter, the site of origin from the aorta, distance of each accessory artery from the main renal artery and classifying each accessory artery as hilar or polar. A hilar artery is one that enters at the hilum and a polar artery is the one that reaches the pole. A kidney with an inferior accessory polar artery is generally avoided as the polar artery generally supplies the renal pelvis and proximal ureter and ligating/thrombosis of this vessel can cause stricture formation or urinary leak.
3. Segmental bifurcation of the main renal artery – It is important to measure the distance of the main bifurcation of the right renal artery from the aorta and also the right margin of the inferior vena cava (IVC); distance of the segmentary bifurcation of the left renal artery from the aorta.
Early segmental bifurcation (within 1 cm from origin) is generally not preferred as a donor candidate because vascular anastomosis will become complex – the pedicle will not be long enough to allow for an easy anastomosis.
If there are more than one artery then surgeons also need the measurement of the distance between the two arteries and the distance before the segmentary bifurcation. This will help them decide how to anastomose them to the recipient arteries.
4. Accessory renal veins – knowledge of the location and diameter of renal vein tributaries is important especially in laparoscopic donor nephrectomy.
5. Distance of confluence of right renal vein to the IVC (early confluence is <15 mm from IVC).
6. Distance of confluence of left renal vein to IVC and from aorta (early confluence is <15 mm from the left aortic margin).
7. Circum- or retro-aortic variants of renal veins
In a meta-analysis published in 2019, Hostiuc et al. looked at 105 articles (more than 47,000 patients) and found that the prevalence for retroaortic renal vein was 3% (CI 2.4%–3.6%), and that of circumaortic renal vein was 3.5% (CI 2.8%–4.4%). He also found that the prevalence for multiple renal veins – 16.7% (CI 14.3%–19.2%), eight times more frequently found on the right.
Pandya et al. in their study of CT angiogram for preoperative workup for potential live renal donors found that the standard pattern of drainage of renal veins occurred in 67% of donors on the right side and 92% of donors on the left side. They classified the variations on the left side as supernumerary (1%), retroaortic (2.5%), circumaortic (4%) and plexiform (0.5%).
A kidney with double right renal vein or circumaortic left renal vein is not preferred as donor.
8. IVC anomalies
9. Atherosclerosis of the donor renal artery – Now with the expanded donor criteria, it is not uncommon to see older donors with atherosclerotic vessels. It generally involves the origin or proximal part of the renal artery. If the donor has unilateral renal artery disease, then true kidney with the atherosclerotic plaque is harvested and the plaque may be either tacked to the wall or the involved segment resected during bench dissection. Calcified plaques make it difficult for the surgeon to apply the vascular clamps safely and this can lead to plaque rupture, distal embolization or troublesome bleeding. Hence, the presence of plaques in the donor artery and aorta; and whether it is a soft or calcified plaque should be mentioned in the report. Presence of bilateral renal artery atherosclerotic disease is generally an exclusion criteria for donation. Calcium scoring systems and calcification morphology especially in patients with advanced age and diabetes have also been proposed to help in selecting which side iliac vessels should be selected for anastomoses.
10. Fibromuscular dysplasia – this nonatherosclerotic noninflammatory disease affects renal and carotid vessels in young women and is characterized by the classical ‘string-of-beads’ appearance on CTA. There is an incidence of 2%–5% in asymptomatic living donors. If detected as unilateral disease, the affected kidney may be chosen for donation and the involved segment resected and replaced with a graft (synthetic or biological) for the anastomosis if needed. Bilateral disease is an exclusion for donation. However, it is important to rule out respiratory artefacts which may mimic fibromuscular dysplasia. If needed, angiography may be done.
Preoperative assessment of the recipient
Specific history pertinent to avoiding intraoperative surprises include:
1. History of any femoral artery or vein indwelling catheters or dialysis catheters
2. History of DVT in the past
3. Hypercoagulable disorder
Imaging of the recipient
Doppler of the iliac arteries and veins
1. DVT and sequelae – the side of the DVT will be avoided for the graft. Opposite iliac fossa and iliac vessels will be preferred.
2. Atherosclerosis or vasculitis involving the iliac and femoral arteries.
3. Size of the internal iliac artery if possible.
4. Any reason for compromise of space in the iliac fossae for placement of the graft like soft tissue masses, scarring from a previous surgical incision or polycystic kidneys.
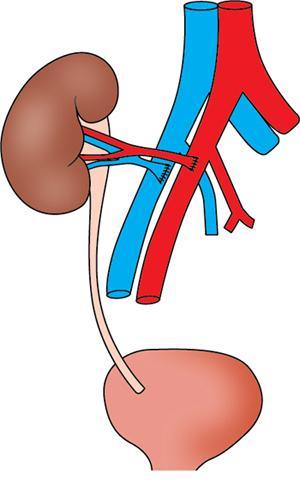
Vascular anastomoses are easier to perform on the right side because of the superficial and horizontal course of the right iliac vein. When the kidneys are harvested from a cadaveric donor, often there is an intact main renal artery and other accessory branches along with an attached portion of the aorta (Carrel patch) and this is typically anastomosed end to side of the recipient external iliac artery (EIA). In the case of a living donor, harvesting a section of the aorta is not possible. Hence, either an end to side anastomosis of the donor renal artery is done to the recipient EIA or an end-to-end anastomosis is done to the recipient internal iliac artery (IIA). The donor renal vein (cadaveric or living) is sutured end to side to the recipient external iliac vein (EIV) (Figs. 10.22.1.1–10.22.1.8).
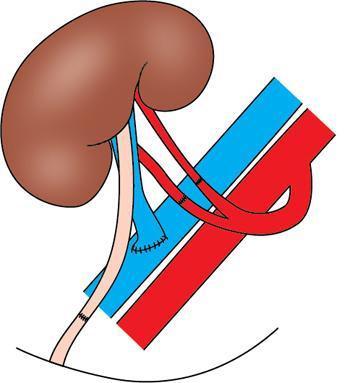
Fig. 10.22.1.1This depicts the standard renal transplant anastomosis. The donor artery is anastomosed end-to-side to the CIA and the donor vein is anastomosed end-to-side to the CIV.
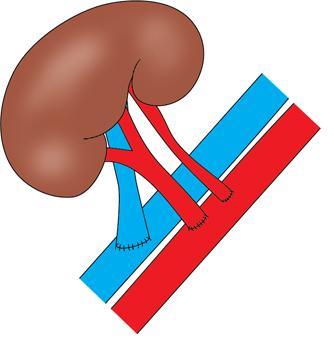
Fig. 10.22.1.2Main and accessory renal artery anastomosis to right exteranal illiac artery.
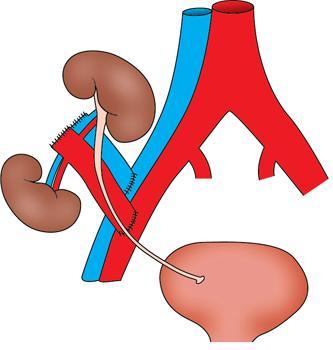
Fig. 10.22.1.3Dual kidney transplant in right illiac fossa.
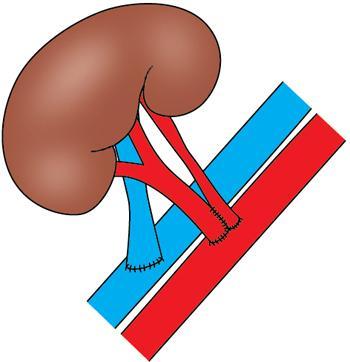
Fig. 10.22.1.4Main and accessory renal artery combined anastomosis to right exteranal illiac artery.
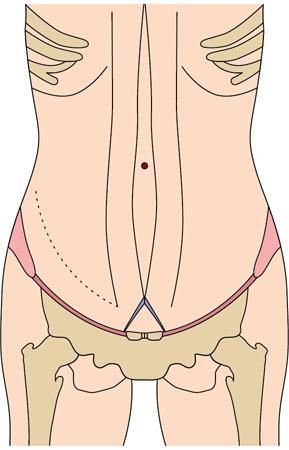
Fig. 10.22.1.5Standard incision in the right iliac fossa for a renal transplant.
Fig. 10.22.1.6If there are 3 renal arteries, then this is considered. One renal artery to the anterior division of the IIA, second renal artery to the posterior division of the IIA and the third renal artery to the inferior epigastric artery.
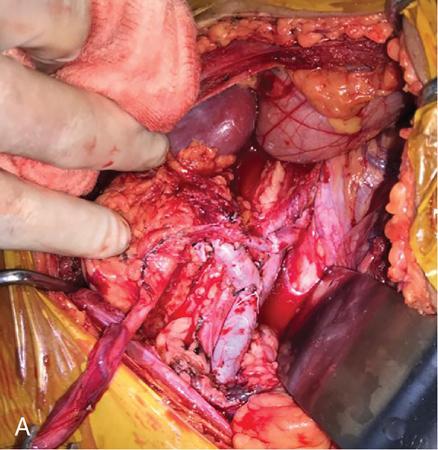
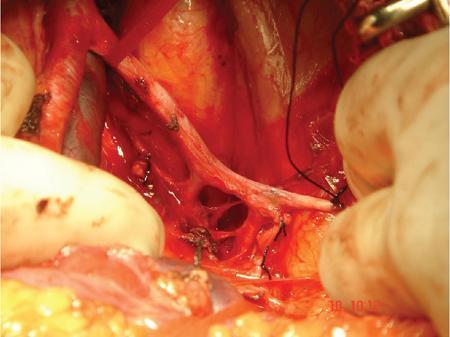
Fig. 10.22.1.7(A) Intraoperative photograph showing the transplanted live donor kidney with renal artery anastomosed end-to-end to recipient IIA (internal iliac artery) and renal vein anastomosed end-to-side to recipient EIV. The ureter is yet to be anastomosed to the bladder. (B) This intraoperative photograph shows live donor kidney where the lower polar artery was missed on a preop conventional angiogram leading to a surprise after harvest. The main renal artery was anastomosed end-to-end to IIA (black arrow) and the smaller polar artery was anastomosed end-to-side to the EIA. The renal vein was anastomosed to the EIV (blue arrow).
Fig. 10.22.1.8This intraoperative photograph in a live donor kidney shows the urine pulsing out of the cut end of the donor ureter as soon as the anastomoses are completed and the clamps are released.
Various surgical combinations that are possible during anastomosis
Arterial anastomoses
1. Renal artery anastomosed end-to-end to the recipient Internal Iliac artery – This is the simplest and most commonly used technique. However, it is not preferred in young patients especially men or if the contralateral Internal iliac artery is diseased.
2. Renal artery anastomosed end-to-side to the common iliac artery (CIA) or external iliac artery (EIA) – CIA will be preferred as the lumen is wider and less chance of stenosis and later claudication to the leg.
3. Multiple renal arteries:
a. If the deceased donor kidney has two or more renal arteries, it is preferable to harvest them with a cuff of the aorta and this can be used to anastomose it to the CIA or EIA as a Carrell’s patch.
b. If Carell’s patch is not possible or it is a live donor kidney, then the various options are:
• Both the renal arteries can be anastomosed separately end-to-side to the CIA.
• The main renal artery can be anastomosed to the CIA. The smaller renal artery can be anastomosed to the IIA or the inferior epigastric artery.
• The two ostia of the renal arteries can be combined in a barrel shape and then anastomosed end-to-side of the CIA.
• The smaller renal artery can be anastomosed end-to-side of the main renal artery (this will be done as part of the bench dissection and preparation – part of cold ischaemia time). The main renal artery is then anastomosed end-to-side of CIA.
• Sometimes, an experienced transplant surgeon can dissect out and divide a suitable length of the recipient IIA with the bifurcation into the anterior and posterior divisions. This is then anastomosed to the two renal arteries during the bench dissection and preparation – where it is easier to do the anastomosis compared to the depth of the pelvis in the operating field. This graft is now anastomosed to the CIA to the patient.
Venous anastomoses
1. Renal vein is anastomosed end-to-side to the CIV. Sometimes especially when it’s the right donor kidney with a short right renal vein, the recipient internal iliac vein and other branches are ligated to mobilize the CIV and make it easier to do the anastomosis. This however has to be done carefully because if the distal end of the branches or IIV slips then it can lead to troublesome bleeding in the pelvic depth.
2. Sometimes when the renal vein length falls short, an interposition graft using great saphenous vein or cryopreserved cadaveric iliac artery graft may be prepared and used to anastomosed to the CIV.
3. Two renal veins can be anastomosed separately on to the CIV.
4. If there are small accessory renal veins, they can be ligated. Unlike arteries, small collateral vessels develop between the veins and flow is redirected thus preventing renal venous infarcts.
Intraoperative assessment
Once the anastomoses are done and the graft is opened to the recipient’s systemic circulation, an assessment is made to decide whether the graft is functioning. A clear answer can be made if there is peristalsis in the graft ureter and urine is seen pulsing out of the cut end of the ureter. Other signs are that the graft will turn pink and firm to touch and there will be a palpable thrill at the hilum over the renal artery.
However, there are times when these signs are absent or equivocal. Risk factors for this are hypotension in the recipient, paediatric recipients with small vessels, complex vascular reconstruction, diseased donor or recipient vessels.
If after trying measures like volume loading of the patient, papaverine injection locally to dilate the arteries, the graft colour and feel does not improve or brisk urine production does not start, then further assessment to assess the flow across the anastomoses is considered.
Intraoperative assessment
1. Intraoperative indocyanine green (ICG) imaging can be used.
2. Doppler to assess patency of the arterial and venous anastomosis and iliac vessel flow. Resistive index of <0.5 was suggested as an index for surgical revision of the anastomosis.
Postoperative assessment
1. Suspected bleeding in the immediate postoperative period – whether it’s a leak from the anastomosis or a collection due to diffuse oozing secondary to deranged coagulation profile.
2. Decreasing urine output and rising creatinine.
3. Suspected graft rejection.
Imaging for the transplanted kidney
1. Colour Doppler
2. CT angiogram
3. MR angiogram gadolinium
4. MR angiogram unenhanced
SLEEK – it is a respiratory triggered three-dimensional fat saturated fast imaging employing steady state acquisition prepared with multiple spatial selective inversion recovery pulses. However, this requires respiratory training for the patient. Tang et al. have reported their results with 75 transplanted kidneys and found an excellent positive correlation between findings on SLEEK with that on DSA and surgery. They found that SLEEK picked up more accessory renal arteries than colour Doppler which could not pick up vessels below 3 mm. They also found that though SLEEK gave a slight overestimation of the magnitude of renal artery stenosis as compared to DSA, it was not statistically significant.
Postoperative vascular complications
Postoperative complications can occur in up to 12%–20% of patients undergoing renal transplantation, vascular complications up to 15%.
These can be catastrophic and if not timely detected and treated, can result in loss of graft and/or the ipsilateral limb. It is important to differentiate these from rejection or drug toxicity as the management varies greatly.
Risk factors for vascular complications
1. Age – extremes of age such as less than 10 and more than 65 years old have higher incidence of vascular complications.
2. Gender – females tend to have more thrombotic complications.
3. BMI – higher BMI has higher incidence of complications.
4. Living versus deceased donor – deceased donor kidneys have higher warm ischemia time and higher risk of complications.
5. Presence of multiple accessory vessels – it makes the vascular reconstruction more complex and increases the risk of complications.
6. Recipient vessel atherosclerosis or calcification – it makes clamping sometimes difficult.
7. Difficult bench surgery – in the repair of injuries or in preparation for a complex vascular reconstruction increases the risk of vascular complications.
8. Use of antiplatelet or anticoagulant drugs in the perioperative period.
9. Each month on dialysis – increases platelet dysfunction and other coagulation abnormalities which increases the risk of bleeding.
10. Immunosuppressants like sirolimus can cause increase in thrombotic complications.
11. Retransplants – due to the scarring and difficult dissection can result in intraoperative and postoperative bleeding.
Only gold members can continue reading. Log In or Register to continue