Fig. 2.1
Positioning of the ultrasound system in the operative theater: the operator faces the screen, which can be managed by the second or third assistant

Fig. 2.2
An ultrasound system with a sterile pad covering the keyboard to allow its management by the surgical team directly
After entering the abdominal cavity and preceding IOUS exploration, the liver should be mobilized dividing the round and falciform ligaments (Fig. 2.3a) and eventual adhesions should be dissected to free the anterosuperior and inferior surfaces of the liver (Fig. 2.3b). Of course, adhesions with other organs or structures should not be severed as to possible tumor infiltration. In that case, IOUS can be helpful in ruling out or confirming the tumor invasion and allow for changing the surgical strategy accordingly. Palpation of the organ needs to precede the exploration with IOUS; indeed, as recently demonstrated [1], inspection and palpation of the liver are still of paramount importance.
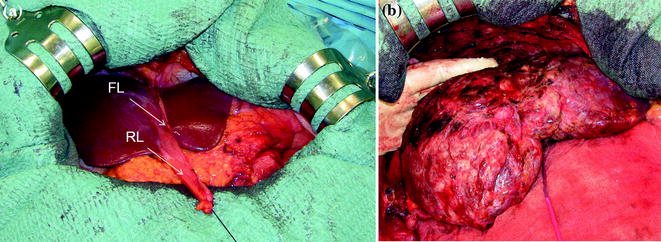
Fig. 2.3
a The liver is exposed for initial exploration once the falciform ligament (FL) has been cut and the caval confluence has not been exposed yet for avoiding artifacts upon IOUS; b liver exposed after extensive adhesions have been removed; round ligament (RL)
By pulling the round ligament, the liver surface is widely exposed and following the portal branches and the hepatic veins, the liver can be entirely studied (Fig. 2.4). The probe should be managed using a pressure sufficient to ensure a good contact with the liver surface but not to compress the intrahepatic vascular structures and in particular the hepatic veins. Generally, at the onset one should not move the probe extensively over the liver surface but identify a vascular landmark which is generally represented by the main portal bifurcation. Then, once identified (see Chap. 3), just a minimal shifting of the probe on the liver surface would allow following all the portal pedicles, and exploring all liver segments by IOUS (Fig. 2.5a, b).

Fig. 2.4
A surgeon handling a probe and initially exploring the liver; round ligament (RL)
Fig. 2.5
Moving the probe while exploring the liver. This consists in minimal upward and downward tilting (a) or rotation (b) of the probe, avoiding its extensive shifting on the liver surface
The hard and irregular surface of cirrhotic liver (Fig. 2.6), scars due to previous resection or strong adhesions in reoperated patients (Fig. 2.3b), or simply a heterogeneous ultrasound pattern make it somewhat difficult to detect small nodes both by palpation and IOUS exploration. Under such circumstances, searching a scanning window opposite the site of an unsuitable exploration to provide a deeper access than the initial superficial one would be essential to increase the chance to detect these lesions by IOUS (Fig. 2.7a, b). This maneuver can be further improved by keeping the fingertip on the liver surface opposed to that in contact with the probe, paying attention to match the fingertip plane with that of the scanning window (Fig. 2.7c, d).
Get Clinical Tree app for offline access
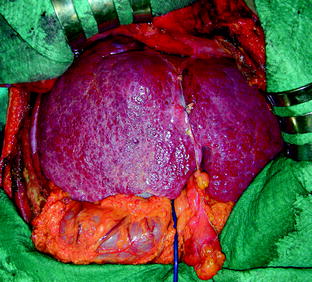
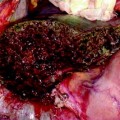
Fig. 2.6
Cirrhotic liver after initial exposure
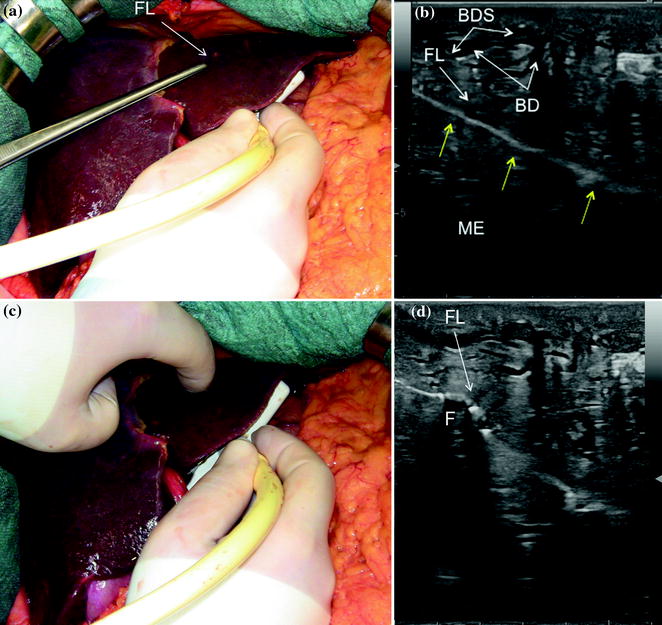
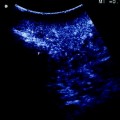
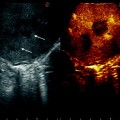
Fig. 2.7
Procedure of scanning superficial lesions without adopting water-filled gloves (see also Chaps. 1 and 4). The lesion visible at inspection (FL), indicated by the forceps, is searched for ultrasound confirmation having the probe scanning at the opposite side (a). In this case, the lesion could not be confirmed with certainty due to inhomogeneous liver bile duct dilation (BD) and the presence of biliary sludge (BDS) (b). For this reason a simultaneous finger palpation of the lesion (c), concurrently with IOUS, enables to precisely put in relation the suspected lesions at IOUS with the surgeon’s fingertip (F
 Liver Transplantation from Living Donors
Liver Transplantation from Living Donors
 Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
 Laparoscopic Ultrasound: Impact in Liver Surgery
Laparoscopic Ultrasound: Impact in Liver Surgery
 Technological Requirements for Ultrasound-Guided Liver Surgery
Technological Requirements for Ultrasound-Guided Liver Surgery
 Exploring the Liver by Ultrasound Along its Anatomy
Exploring the Liver by Ultrasound Along its Anatomy
 Liver Transplantation from Deceased Donors
Liver Transplantation from Deceased Donors




Related posts:
Liver Transplantation from Living Donors
Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
Laparoscopic Ultrasound: Impact in Liver Surgery
Technological Requirements for Ultrasound-Guided Liver Surgery
Exploring the Liver by Ultrasound Along its Anatomy
Liver Transplantation from Deceased Donors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
