, Yves Etienne2 and Maurice Niddam3
(1)
Faculté de Médecine, Marseille, France
(2)
Unité de Médecine Légale, Hôpital de la Timone, Marseille, France
(3)
Unité SAMU 13, Centre 15, Hôpital de la Timone, Marseille, France
This dissection is performed on a half-brain, preferably prepared by a post-mortem injection of embalming fluid with formaldehyde 10 %1 (which is the only product capable of ensuring an effective preservation and consistency of the nerve tissues, therefore allowing dissection without any decaying).
It is at the level of the medial surface of the temporal lobe that the amygdalo-hippocampal area is identified. It is hidden in the front region by multiple vessels located at the terminal arborisation of the internal carotid artery and whose small branches seem to intermingle before penetrating the anterior perforated substance and in the rear region by half of the brainstem that, in general, has been preserved with the hemisphere to be dissected and which is difficult to retract. Therefore, the first part of the dissection involves removing the brainstem by making an incision in the mesencephalon with a scalpel and eliminating the fine vascular network and the arachnoid’s remains that hinder the vision of the area of interest. On the other hand, we will retain, as far as possible, the vessels of the arterial circle of the base which are important references.
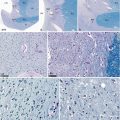
We therefore obtain the view shown in picture a (Fig. 5.1), where the most important characteristics appear: the sectioned internal carotid, the uncus of the hippocampus, the temporal pole and in front of the anterior perforated substance (apSB), the orbital surface of the frontal lobe, under which is routed the olfactory tract.
Fig. 5.1
Dissection of the amygdaloid complex (successive stages). (a) Initial aspect (medial view of a right half-brain). (b) Cortical temporal window Aco anterior commissure, apSb anterior perforated substance, Chpl choroid plexus, Cif cingulate fasciculus, ColS collateral sulcus, crCe crus cerebri, eAr entorhinal area, erS endorhinal sulcus, Fb fornix body, Fc column of the fornix, flV3 floor of the third ventricle, G band of Giacomini, GA gyrus ambiens, GR gyrus rectus, HyS hypothalamic sulcus, IC internal carotid, iThad interthalamic adhesion, lOTG lateral occipitotemporal gyrus, MB mammilliary body, Mes mesencephalon, olt olfactory tract, OrG orbital gyri, ot optic tract, patG paraterminal gyrus, PB pineal body, pHG parahippocampal gyrus, pHG’ (pL) anterior part of the pHG (piriform lobe), ppc pre-piriform cortex, rhS rhinal sulcus, sCG subcallosal gyrus, slG semi-lunaris gyrus, splCC splenium of the corpus callosum, TOL temporal lobe, Tpo temporal pole, UG uncinate gyrus, Un a uncus apex, Unn uncal notch, UnS uncal sulcus, V3 third ventricle, a1 anterior cerebral artery, a2 middle cerebral artery, a3 posterior cerebral artery, II optic nerve, white arrowhead interventricular foramen (ivf), black arrowhead semi-annular sulcus (sas)
At the level of the uncus, it is possible to observe the underlying uncal sulcus and the band of Giacomini, which borders, in the front region, the apex of the uncus. Further down, another major sulcus borders, in a downward direction, the area to be dissected: this is the perirhinal sulcus, above which the cortex forms a large and almost flat area, the entorhinal area. It is above this area that we can observe the gyri belonging to the periamygdaloid cortex: from back to front, the semilunar gyrus and the gyrus ambiens, separated by the sulcus semi-annular or amygdaloid sulcus, and then at the level of the uncus (hence its name), the uncinate gyrus.
The next phase involves creating a cortical window in order to view the above area. We will also make sure that a large cortical surface is not immediately resected in order to retain the overall architecture. Cortical resection will remove, on the one hand, all of the medial surface of the periamygdaloid cortex (with the exception of the cortical band which borders the deep endorhinal sulcus) but also the upper three quarters of the entorhinal cortex and impact the uncinate gyrus while remaining at ¼ cm from the anterior edge of the band of Giacomini. This band marks the border area between the upper digitation of the head of the hippocampus and the superior pole of the amygdala. Once the cortical window is created, picture b (Fig. 5.1), it is observed that the amygdala is still not visible: a fibrous wall is present and appears as a thick white rectangular band, which can be easily separated from the cortex which covers it. This band is the inferior end of a large and remarkable white substance pathway: the cingulate fasciculus (see Chap. 7). It is noted that the pathway bends when it reaches the amygdala, such as a protective shield (see Fig. 7.15).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


