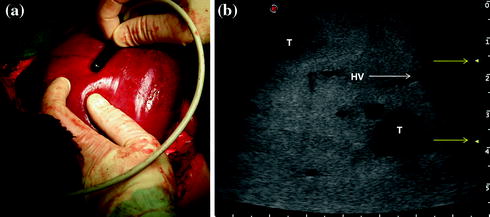
Fig. 1.1
a A convex probe for percutaneous exploration, used intraoperatively for an initial overview, and for cases where an improved panoramicity of the exploration is needed. Particular features: relatively low frequency, possibility to depict deep structures though loosing in spatial resolution; b A convex-probe scan: one scan reveals a tumor (T) in the liver, right hepatic vein (RHV), retrohepatic inferior vena cava (IVC), and diaphragm (D)

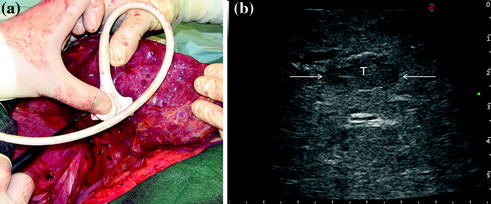
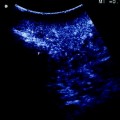
Fig. 1.2
For better exploration of the superficial structures, a glove filled with deaerated water (G) is positioned between the probe and the targeted surface; arrows indicate a small lesion (T)
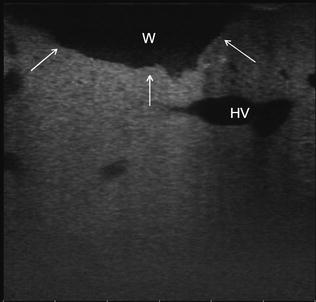
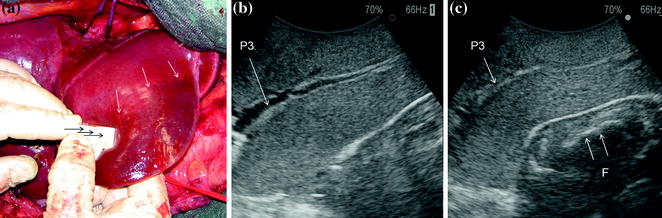
Fig. 1.3
The cut surface (arrows) can be explored by filling the cavity with deaerated water (W); hepatic vein (HV)
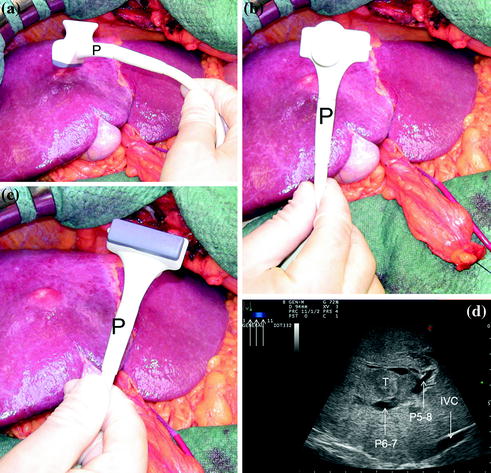
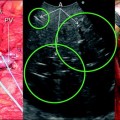
Fig. 1.4
Profile (a), dorsal (b), and scanning side (c) of a micro-T-shaped linear echoprobe (Esaote SpA, Genova, Italy) designed for surgical maneuvers, featuring a trapezoid scanning window and a wide (3–11 MHz) range of frequencies (arrows) (d); tumor (T); portal branch to segments 5 and 8 (P5-8); portal branch to segments 6 and 7 (P6-7); inferior vena cava (IVC)
A crucial point to be evaluated while selecting a probe is its shape and volume. Indeed, an optimal probe should represent the best compromise between the size, which should be small to allow its handling in deep and narrowed spaces, and the ultrasonographic scanning window, which should be large enough to provide a widest possible area of exploration in a single view; the adherence to the surface of the target organ should be high enough for enabling an adequate stability along its handling and for avoiding gas interposition, reducing the number of possible artefacts in organ exploration. The most frequently used probes are T-shaped with linear (Fig. 1.5a, b) or convex scanning head (Fig. 1.6a, b), interdigital (Fig. 1.7a, b), and microconvex (Fig. 1.8a, b). The microconvex probe provides the best solution regarding the aforementioned desirable criteria. Indeed, the T-shaped probe, while remaining more stable and being associated with higher image resolution, has a lower ratio between lateral length and ultrasonographic scanning window than the microconvex one. Linear transducers, with enlarged scanning windows, have more recently become available (trapezoid scanning window): these combine the stability of the linear probes and their higher image resolution with larger scanning windows and a limited volume (Figs. 1.4a–d, 1.9a, b). Another aspect to be considered in evaluating a probe is whether it can be used for surgical maneuvers as those described in Chap. 8 for which the echoprobe is acting as a kind of surgical instrument (see Fig. 1.10a–c).
Get Clinical Tree app for offline access
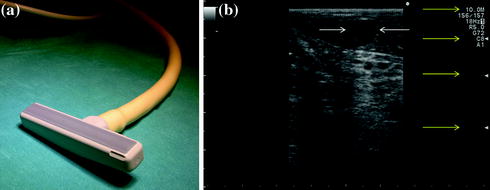
Fig. 1.5
a The scanning side of a T-shaped linear echoprobe (Hitachi-Aloka Medical; Tokyo, Japan); b the scanning area is also disclosed and a small lesion (cyst) is shown: this high-frequency echoprobe (5–10 MHz) is featured by a high resolution but a low power of ultrasound penetration, which means relatively limited panoramicity. The yellow arrows indicate from top to bottom the frequency at which it is working in that precise moment (10 MHz) and the three focal levels
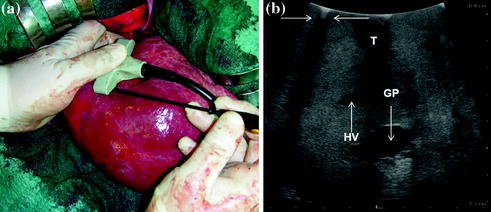
Fig. 1.6
a The scanning side of a T-shaped convex echoprobe (BK Medical APS, Peabody MA, USA) with an electrocautery positioned between the liver and the probe; b the scanning area is also disclosed and a small lesion (T) is shown together with the posterior echo (arrows) generated by the tip of the electrocautery; glissonian pedicle (GP); hepatic vein (HV)
Fig. 1.7
a A interdigital linear echoprobe (Esaote SpA, Genova, Italy); b the trapezoid scanning area is also disclosed and two lesions (T) are shown. Yellow arrows indicate the two focal levels; hepatic vein (HV)
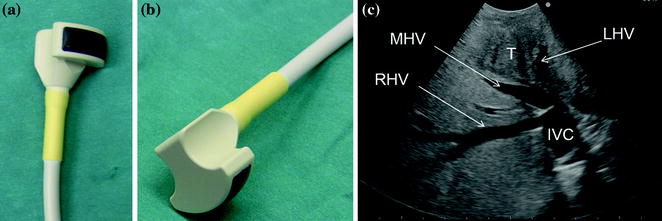
Fig. 1.8
The scanning side (a) and opposite side (b) of a microconvex echoprobe (Hitachi-Aloka Medical; Tokyo, Japan). The scanning area is also disclosed (c) the wide-frequency-range echoprobe (2–7 MHz) in one scan shows the liver with a tumor (T)—right (RHV), middle (MHV), and left (LHV) hepatic veins are recognizable; inferior vena cava (IVC)
Fig. 1.9
An intraoperative micro-T-shaped linear probe (Esaote SpA, Genova, Italy) (a). Featuring a trapezoidal scanning window (b). This probe combines the stability of a linear transducer and the wideness of the scanning window of a convex probe. It was designed also for allowing ultrasound-guided compressions maneuvers (see Chap. 8); tumor (T)
Fig. 1.10
a
 Liver Transplantation from Living Donors
Liver Transplantation from Living Donors
 Technical Tricks to Start Exploring the Liver with Ultrasound
Technical Tricks to Start Exploring the Liver with Ultrasound
 Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
 Intraoperative Cholangio Ultrasound in the Study of the Biliary Tree
Intraoperative Cholangio Ultrasound in the Study of the Biliary Tree
 Exploring the Liver by Ultrasound Along its Anatomy
Exploring the Liver by Ultrasound Along its Anatomy
 Liver Transplantation from Deceased Donors
Liver Transplantation from Deceased Donors




Related posts:
Liver Transplantation from Living Donors
Technical Tricks to Start Exploring the Liver with Ultrasound
Diagnosis and Staging: Contrast-Enhanced Intraoperative Ultrasound (CEIOUS) Using Intravascular Contrast Agents
Intraoperative Cholangio Ultrasound in the Study of the Biliary Tree
Exploring the Liver by Ultrasound Along its Anatomy
Liver Transplantation from Deceased Donors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
