Cryptorchidism or undescended testes (UDT) is failure of one or both testicles to descent into scrotal sac. Normally testicular descent occurs between 7th and 8th months of gestational age. Approximately 30% of premature and 3.4% full-term male infants have a UDT. Spontaneous descent occurs in 50%–70% cases by the end of 3rd month. Cryptorchidism is more common on right side (70%) and is bilateral in 10%–33% of cases. Clinically empty ipsilateral scrotal sac is seen. Cryptorchid testis may be palpable (canalicular) or nonpalpable (intraabdominal). The current standard of therapy is surgical repositioning of the testis within scrotal sac (orchiopexy) and hormonal manipulation. Despite successful relocation surgery, infertility, subfertility, and malignancy may occur as a long-term sequela.
Types of cryptorchidism
Cryptorchidism can be congenital, acquired (or ascending testis) and iatrogenic (trapped testis).
Congenital cryptorchidism
• Intraabdominal: located deep to internal ring and in abdominal cavity
• Canalicular: located within inguinal canal
• Suprascrotal: Testicle is seen lodged at or just caudal to superficial inguinal ring at suprascrotal area
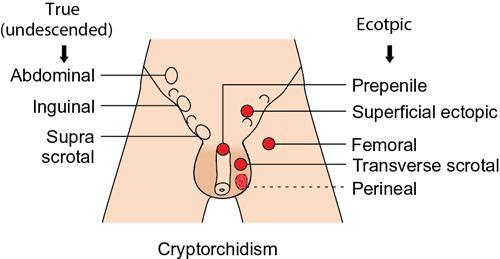
• Ectopic: Testicle located outside and away from its normal path of descent. The various locations for ectopic testis are perineum, femoral canal, superficial inguinal pouch (most common), suprapubic area (prepenile) and opposite hemiscrotum (transverse scrotal position) (Figs. 11.8.1–11.8.2).
• Retractile: It is normally descended scrotal testicle that is hypermobile and moves freely between scrotum and groin.
• Hypoplastic: Testicle is either poorly developed or dysgenetic or vanishing
• Anorchia: Developmentally absent testicle
Fig. 11.8.1Diagrammatic representation of various types of undescended and ectopic testes.
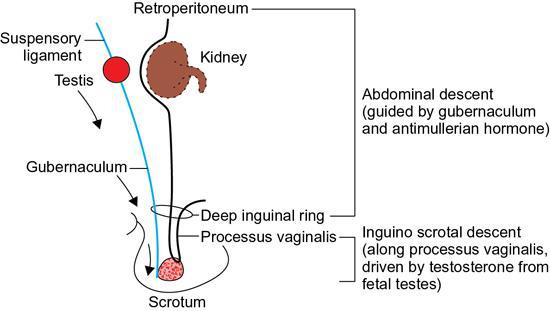
Fig. 11.8.2Diagrammatic representation of normal testicular descent.
Acquired cryptorchidism (ascending testis)
It is ascent of a previously descended testis under the influence of aberrant androgen signalling with prevalence of 1%–7% and peaks around 8 years of age.
Iatrogenic cryptorchidism (‘trapped’ testes)
It is trapping of previously descended testis in scar tissue above the dependent scrotum after inguinoscrotal surgery.
Etiopathogenesis
The aetiology of cryptorchidism is not completely known. However, it may involve abnormalities in mechanical factors (gubernaculums, length of vas, testicular vessels, cremasteric muscles and abdominal pressure), abnormal hormonal stimulation and reception factors (gonadotropin, testosterone and Mullerian inhibiting substance), neural factors (ilio- and genitor-femoral nerves), or combination of these
Risk factors implicated in cryptorchidism are family history, low birth weight (prematurity) and retractile nature. Other commonly associated conditions are inguinal hernia, hydrocele, intersex disorders, hypogonadotropic hypogonadism, Prune-belly syndrome, meningomyelocele, hypospadias, Wilms’ tumour and cystic fibrosis.
Laboratory investigations
In phenotypic male newborn with bilateral nonpalpable UDTs, hormone levels (LH, FSH, MIS [Mullerian inhibiting substance] and testosterone) are helpful to determine presence of testis.
Diagnostic imaging
USG: High-resolution colour Doppler ultrasound is the modality of choice for identification and localization of cryptorchid testis as it is easily available, cost effective and radiation free.
USG findings include empty scrotal sac with UDT usually small, iso- or hypoechoic relative to normal testis. Palpable UDT is most frequently seen in inguinal canal or suprascrotal region just caudal to external inguinal ring (Figs. 11.8.4–11.8.6). Retractile testis at suprascrotal location can be brought down by probe manoeuvre.
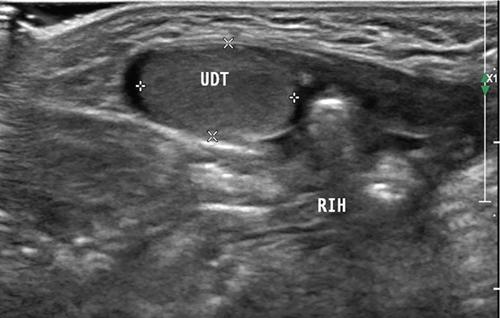
Fig. 11.8.3Inguinal US scan of a 2-month-old male child shows undescended right testis (UDT in cursors) at superficial inguinal ring with associated inguinal hernia (RIH). Clinically the child presented with empty right hemiscrotum since birth.
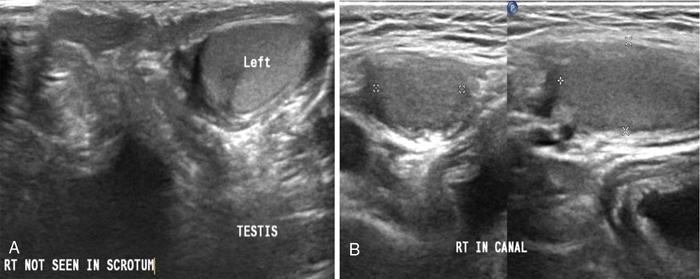
Fig. 11.8.4(A) Scrotal US scan of a 7-year-old male child shows absent right testicle in ipsilateral hemiscrotum, and (B) US scan of right inguinal region shows presence of testicle in inguinal canal (canalicular UDT).
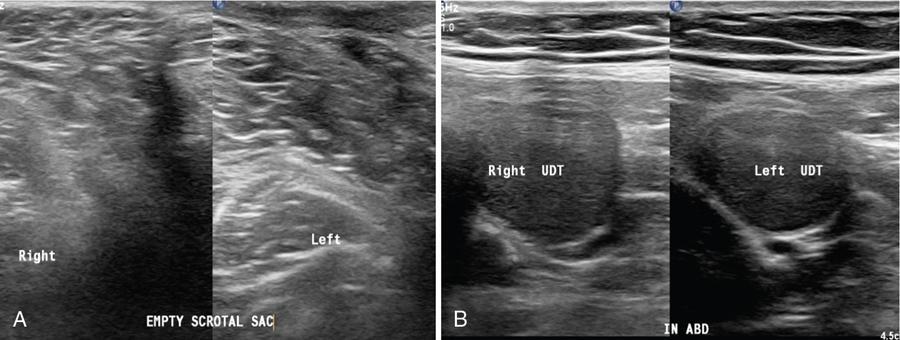
Fig. 11.8.5(A) Scrotal US scan of a 25-year-old male shows absent of both right and left testicles in respective hemiscrotal sacs (empty scrotal sac, s/o bilateral UDT). (B) Suprapubic US scans of the same case of empty scrotal sac showing both right and left testicles lodged in abdominal cavity traced on either side of urinary bladder (bilateral intraabdominal UDT).
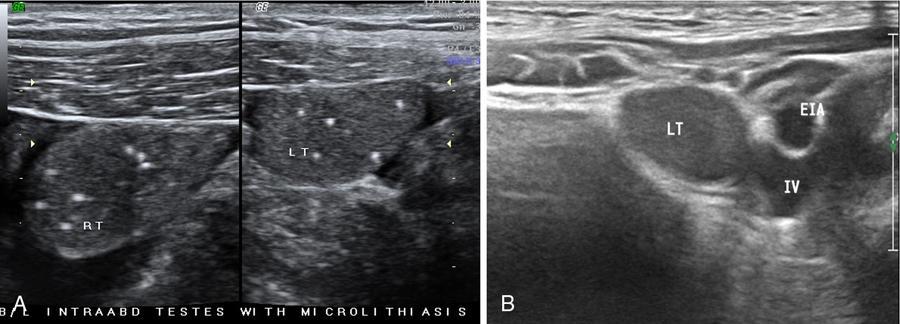
Fig. 11.8.6(A) Suprapubic US scan of a 22-year-old male with empty scrotal sac shows bilateral small-sized intraabdominal UDT with microlithiasis. (B) Another case showing intraabdominal undescended left testis (LT) adjacent and medial to iliac vessels and abutting urinary bladder wall.
Visibility of nonpalpable intraabdominally located testis is impaired by bowel gases at US, however, with experienced hands the same can be depicted on ultrasound deep to internal inguinal ring, adjacent to iliac vessels and lateral bladder wall. Tracking the cord technique is also a valuable sign in localizing nonpalpable testis (also ectopic testis) (Fig. 11.8.3).
Intraabdominal testis is more prone for malignant transformation whereas canalicular testis for torsion (bulky heteroechoic testis, devoid of internal vascularity, with adjacent whirlpool sign or mass). In canalicular torsion testis the child usually presents with acute painful groin swelling (Figs. 11.8.7–11.8.8).
CT: In the early 1980s, Lee et al. reported that CT accurately localized 100% of eight UDT; though five of these were palpable in the inguinal canal. As CT scan includes potential risk of secondary malignancies due to ionizing radiation, we believe that there is no role for routine CT evaluation of boys with UDT. However, it has an important role in staging of testicular malignancy in boys with cryptorchidism.
MRI: As compared to CT scan (which involves ionizing radiation) and ultrasound, MRI has greater diagnostic accuracy to assess cryptorchidism. It almost replaced CT, and is higher sensitive and specific than ultrasound in evaluation of nonpalpable testes in equivocal cases. The sensitivity of MRI falls between 85% and 89.5% (with DWI) with specificity up to 100%, as compared to 21%–76% with ultrasound. As for as MR imaging of nonpalpable intraabdominal UDT is concerned, a combination of DWI and conventional MRI has been proved to be more sensitive and a result yielding technique. At conventional MR the UDT is seen as round to oval mass in the path of it’s descent along gonadal vessels with typical intermediate signal on T1-weighted and homogeneous high signal on T2-weighted sequences, and a hyperintense ovoid structure on DWI.
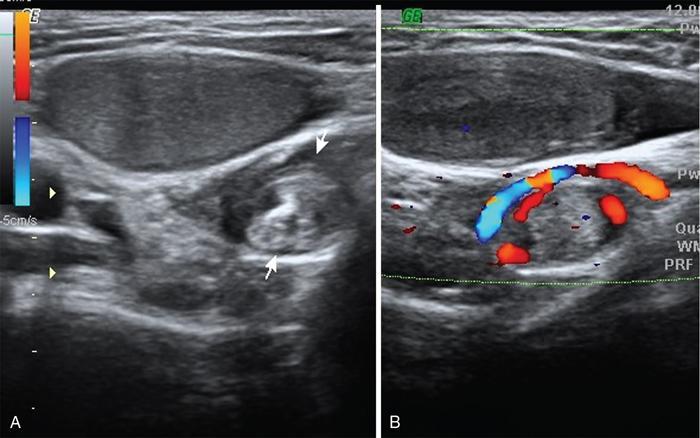
Fig. 11.8.7A 13-year-old male child (known case of palpable right UDT) presented with acute painful swelling right groin area. US and colour Doppler scan of inguinal region shows hypoechoic small-sized undescended right testis at superficial inguinal ring level with twisted spermatic cord in inguinal canal (whirlpool sign between arrows and vascular twist on colour Doppler), s/o torsion of undescended right testis.
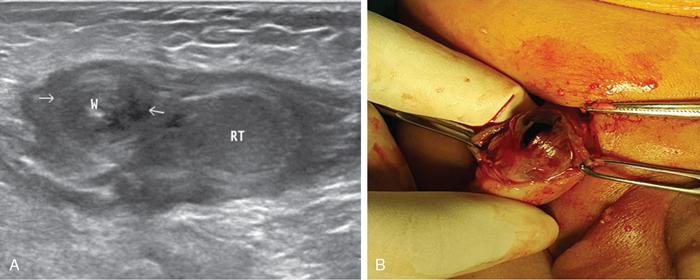
Fig. 11.8.8(A) Right inguinal US scan of a 9-month-old male child showing undescended hypoechoic right testis (RT) in inguinal canal with adjacent spermatic cord twist W (between arrows), s/o torsion of undescended canalicular right testis. (B) Preoperative and gross specimen photographs of the same case showing post torsion infarcted/gangrenous right testis derived from inguinal canal.
Differential diagnosis
• Hypermobile testis (retractile testis) – normally descended testicle that ascends to groin on cremasteric reflex (common in males between 4 and 6 years of age)
• Atrophic testis – may occur due to testicular ischaemia (neonatal torsion)
• Vanished testis – due to poor development or torsion in utero.
Management
It is essential to rule out retractile testis first. In some cases, with a testis close to scrotum, per-scrotal surgical repositioning (orchidopexy) can be performed and often associated inguinal hernia (if present) can also be corrected. In cases with nonpalpable testis, diagnostic laparoscopy allows rapid and safe assessment of intraabdominal testis with single- or two-stage orchiopexy performed in low- and high-placed testicle, respectively. In more difficult situations and in cases of atrophic testis orchidectomy is considered. Testicular prostheses can be used in older children and adolescents for aesthetic purpose and to avoid psychological stigma of empty scrotum. Surgical orchiopexy should be delayed until 18–24 months as spontaneous descent of testis is expected to occur under influence of an endogenous surge of luteinizing hormone. More than 50% cases after orchiopexy are reported to be abnormal on follow-up scans in position, parenchymal architecture, volume and vascular perfusion.
Variations of hydrocele
Introduction
The collection of fluid between the two layers of tunica vaginalis within the scrotum and/or along spermatic cord is called hydrocele.
In male children, hydrocele is the most frequent cause of painless scrotal swelling. Its incidence is about 0.7%–4.7% in male infants and prevalence in adult men is estimated about 1%. Hydrocele is common in newborns and usually disappears without treatment by the age of 1 year. Older boys and adult men can develop hydrocele (acquired) due to infection, inflammation, torsion, trauma and tumour. One to two millilitres of serous fluid can be seen in tunica vaginalis cavity and should not be erroneously diagnosed as hydrocele (Fig. 11.8.9).
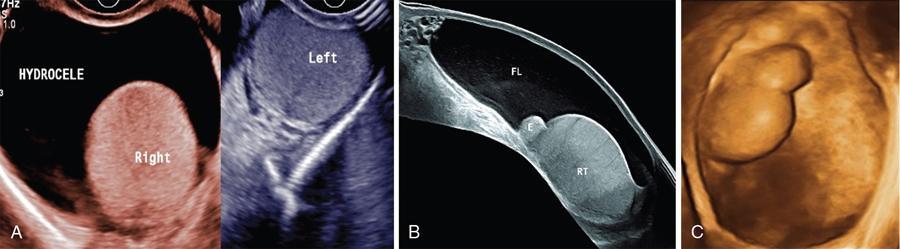
Fig. 11.8.9(A) Transverse US scans of both hemiscrotum showing echo free fluid collection around right testicle (hydrocele). (B and C) Depicting the US Panoramic and 3D images of hydrocele.
Etiopathogenesis of hydrocele
1. Failure of closure or incomplete closure of the processus vaginalis maintaining a communication to the peritoneal cavity or trapping peritoneal fluid anywhere along the length of the tunica vaginalis.
2. Imbalance of production and reabsorption of fluid within tunica vaginalis space in scrotal sac. This disturbance may be a result of infection, tumour, trauma, torsion, defective lymphatic drainage after surgery for varicoceles and inguinal hernias or idiopathic (Fig. 11.8.10).
3. Some risk factors and associated common conditions are renal failure and peritoneal dialysis, nephrotic syndrome, ventriculoperitoneal shunts, testicular tumours and trauma.
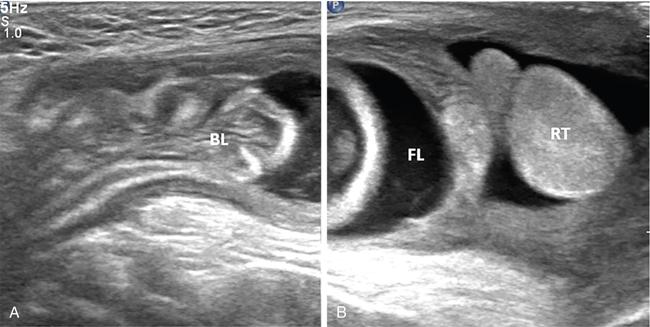
Fig. 11.8.10Combined right inguinoscrotal US images of an infant showing a hernia sac extending up to supra testicular location containing fluid (FL) and herniated bowel loops (BL), consistent with inguinal hernia.
Clinical sign and symptoms
Hydrocele causes acute, subacute or chronic swelling of the scrotum or inguinal canal. Usually all hydroceles are congenital in neonates and infants, and are associated with patent processus vaginalis; whereas hydroceles are mostly acquired in older children and adolescents. Frequent changes in size of hydrocele with position change or activity suggests communicating type. Hydrocele causes painless swelling unless acute in onset. In painful swellings there is sensation of heaviness or pressure in the scrotum or pain radiating to the flank. On physical and examination with light source scrotal swelling is usually fluctuant and transilluminant. A hydrocele that increases in size without an intrascrotal cause suggests the presence of a patent processus vaginalis and the possibility of an associated inguinal hernia (Fig. 11.8.11).
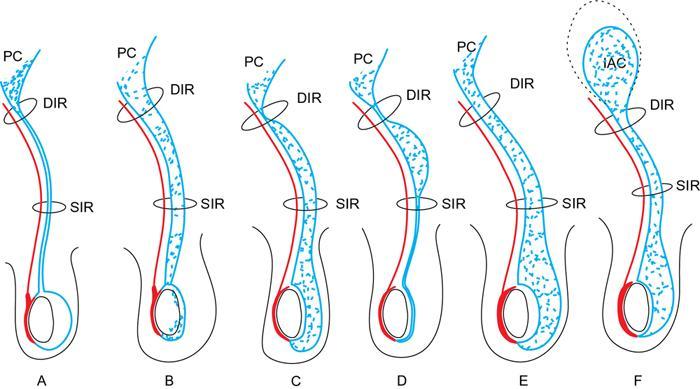
Fig. 11.8.11Diagrammatic drawings depicting various types of hydrocele in males according to abnormalities of patency and obliteration of processus vaginalis. (A) Noncommunicating or scrotal or vaginal hydrocele, (B) funicular hydrocele, (C) inguinoscrotal or infantile hydrocele, (D) encysted hydrocele or spermatic cord cyst, (E) communicating hydrocele and (F) abdominoscrotal hydrocele. PC, peritoneal cavity; IAC, intraabdominal component; DIR, deep inguinal ring; SIR, superficial inguinal ring.
Types (variables) of hydrocele
1] Congenital hydrocele – due to abnormal patency of processus vaginalis ± hernia (Fig. 11.8.11)
2] Acquired hydrocele – usually noncommunicating and based on imbalance between secretion and reabsorption of fluid, and it is of two subtypes:
A] Primary – idiopathic
B] Secondary – to infection/inflammation, torsion, tumour, trauma and postoperative
Classification of congenital hydroceles (in males) (Fig. 11.8.12)
Congenital hydroceles in males can be classified according to the extent of obliteration or patency of the processus vaginalis, into six types and subtypes as follows:
• Communicating Hydrocele – it results when the processus vaginalis is patent in entirety and shows fluid collection that communicates with peritoneal cavity and scrotal sac (Fig. 11.8.13).
• Noncommunicating Hydrocele – it results when the processus vaginalis obliterates but some fluid accumulates between the layers of tunica vaginalis surrounding the testicle in scrotal sac.
• Spermatic Cord Hydrocele – it results when there is abnormal closure of processus vaginalis distally at supratesticular location, leading to a fluid accumulation along the spermatic cord separated from and located above the testis. It comprises of two subtypes.
I. Funicular Hydrocele – it shows fluid accumulation that communicates with peritoneal cavity at the level of deep inguinal ring but does not communicate with tunica vaginalis below in scrotal sac (Fig. 11.8.14).
II. Encysted Hydrocele or Spermatic Cord Cyst – it is seen as cystic lesion along the spermatic cord that neither communicates with the peritoneal cavity above nor with tunica vaginalis below in scrotal sac.
Only gold members can continue reading. Log In or Register to continue