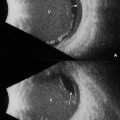
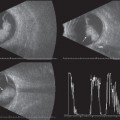
5 Echographic evaluation of choroidal thickening can be very useful in providing a diagnosis or to confirm clinical suspicions in patients with systemic disease. The reflectivity obtained when the sound is aimed through the choroid into the suprachoroidal space is the key echographic finding. Low reflective choroidal infiltration is a significant finding in patients with Vogt-Koyanagi-Harada syndrome (VKH) lymphoid hyperplasia, Lyme disease, sympathetic ophthalmia, or lymphoma. Choroidal thickening that produces high reflectivity is most often associated with processes such as nanophthalmos, uveal effusion, sarcoid, and phthisis. Choroidal detachments most commonly occur following trauma associated with rupture of the globe, trabeculectomy, or as an acute event associated with cataract surgery. Although rare, choroidal detachments have been reported in elderly patients following Valsalva maneuvers such as sneezing, straining, or bending. Ophthalmoscopically, the diagnosis of choroidal detachments can be confusing, particularly if other pathology is present. Certain characteristic echographic features help distinguish choroidal detachments from other intraocular processes. On B-scan, a choroidal detachment appears as a smooth, dome-shaped, thick membrane. Choroidal detachments usually occur in the periphery and may involve the ciliary body (ciliochoroidal detachments). Although they can extend to the posterior pole, they do not insert into the optic disc. Choroidal detachments that involve the entire eye wall, extending 360 degrees, display a typical, scalloped appearance on B-scan. On standardized A-scan, choroidal detachments produce a maximally tall (100%) spike when the sound beam is aligned perpendicular to the surface. This spike is generally thicker than the spike produced by a retinal detachment and is usually double-peaked when there is no overlying retinal detachment. Choroidal detachments may be hemorrhagic or serous in nature and can be mistaken for retinal detachment or mass lesions. Specific echographic features can facilitate the differentiation. Hemorrhagic choroidal detachments will display echo signals beneath the choroidal surface, whereas serous detachments will display an absence of echoes in the suprachoroidal space. On standardized A-scan, a maximally high, 100% tall, thick double-peaked spike will be produced by the retina and choroid together. If the spikes between the choroidal spike and the sclera are low reflective, it is likely that the hemorrhage is more liquefied. However, if these spikes are higher, or more irregular in distribution, the hemorrhage is most likely clotted. Serial ultrasound examinations to evaluate the consistency of the suprachoroidal hemorrhage can be useful to help the surgeon determine when to attempt drainage. On B-scan examination, the density of the suprachoroidal hemorrhage may be less reflective, an indication that the clot has begun to liquefy. Serous choroidal detachments will display a flat baseline between the choroidal spike and the sclera. When bullous detachment of the choroid is present, band formation may be noted beneath the choroidal surface. This suprachoroidal band is thought to be a stretched vortex vein. Echography can be very beneficial in ruling out the presence of “kissing” choroidal detachments (bullous choroidal detachments that meet and touch in the central vitreous space). Kissing choroidals are a serious condition that can lower a patient’s visual prognosis if not treated promptly. Serial ultrasounds are helpful in monitoring the elevation of these detachments during or following treatment. Prolonged low intraocular pressure can lead to hypotony. Echographically, there will be diffuse thickening of the ocular coats and a shortened axial length. If the pressure remains low, scleral infolding may occur. Atta HR, Byrne SF. The findings of standardized echography for choroidal folds. Arch Ophthalmol 1988;106:1234–1241
The Choroid
 Suggested Readings
Suggested Readings
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


