5 The hip and pelvis
History and examination
As with any patient examination, the eliciting of a detailed and accurate history is paramount and lays the foundation for the performance of an appropriate examination and establishment of a working diagnosis and differential. The most crucial element of the history in this area of the body is the precise localization of the area of pain: many patients who complain of ‘hip pain’ do not in fact have pain in their hip and, when questioned, will point to their buttock, gluteal fold or iliac crest; similarly, patients who do have hip pathology will often complain of symptoms in their groin, or the side or front of their thigh – not infrequently described as ‘sciatica’! The use of pain diagrams can help in this regard, but, at the very least, the patient should be asked to point to where they feel pain or discomfort.1,2
With experience, the clinician will normally be able to recognize the atypical presentation of more unusual conditions such as osseous, intrapelvic and spinal lesions. These can, of course, mimic everyday injuries and the clinician should always be alert for an apparently benign condition that fails to respond to normally successful management protocols or is relentlessly progressive. Pain or clicking in the hip of a child is always a cause for concern and usually an indication for diagnostic imaging.3
Associated symptoms such as clicking or popping can also be associated with specific conditions4 and a familial history of pelvic conditions is often very revealing: many conditions such as degenerative coxarthrosis, inflammatory arthropathies, connective tissue disorders and dysplasia have familial tendencies.5–9
Examination should commence with observation of the patient both stationary and walking. Obesity (a body mass index greater than 30) is a significant predisposing factor towards coxarthrosis,10 which will often be accompanied by an obvious flexion contraction causing an inability to stand with a straightened leg on the affected side; other forms of antalgia can also help identify the source of a patient’s pain both in posture and gait.
Although there are myriad orthopaedic tests for the hips and sacroiliac joints, few have any proven validity.11–14 Range of motion, however, often is enough to demonstrate hip pathology, particularly painful reduction of internal rotation. The Patrick/FABER test (external rotation of the hip with the leg in the ‘figure-4’ position: Flexion, Abduction and External Rotation) has been shown to have good reliability as has digital palpation in the identification of greater trochanteric bursitis – the same is also true of the many myofascial trigger points that frequently coexist with pelvic girdle dysfunction and with the posterior margin of the sacroiliac joint.12,15,16
Identification of sacroiliac syndrome is more problematic; however, multiple positive provocation tests have been shown to have a measure of diagnostic reliability; these are detailed in Table 5.0117–19 alongwith tests that the authors have also found useful when similarly used in combination. It is, however, important not to perform too many tests; if three or four have already proved positive, there is little to be gained from continuing and the patient may well have an adverse reaction – the tests are called provocative for a reason and can eventually aggravate the patient’s symptoms. It should also be kept in mind that the pelvis is a closed loop kinematic chain and that comorbidity with lumbosacral facet joint dysfunction is high.20
| Multiple positives are suggestive of sacroiliac injury; if all tests are negative, injury is diagnostically eliminated | |
| Gaenslen’s test | Sit the patient on the edge of a table, flexing one leg to the chest and dropping the other to the floor |
| Compression test | The ilium is forced medially against the sacrum; this is usually done with the patient lying on their side (Figure 5.01) |
| Thigh thrust | The supine patient’s hip is flexed to 90° with the knee bent and a posterior shearing force applied to the sacroilac joint through the femur avoiding hip adduction (Figure 5.02) |
| Distraction test | With the patient lying supine, the anterior superior iliac spines are pressured from lateral to medial |
| Sacral thrust | Posterior to anterior pressure is applied to the sacrum immediately adjacent to the sacroiliac joint |
| Additional sacroiliac joint tests used in combination by the authors with (apparent) success | |
| These tests are not scientifically validated; they do, however, reflect the diagnosis and successful treatment of several thousand sacroiliac joints. The tests have the advantage that they are not all provocative | |
| Yeoman’s test | Forced extension of the sacroiliac joint with the patient lying supine recreating their pain |
| Leg lift Leg lift with cervical compression | If the patient is unable to lift both legs together when locked straight, this is indicative of sacroiliac dysfunction If they are able to perform the above test but find it much more difficult with superior to inferior pressure applied to the top of the head (thus compressing the cervical spine), this is also indicative of sacroiliac dysfunction. Either result is considered as a single positive |
| Piedallu test | The examiner places their thumbs on the posterior superior iliac spines and watches as the seated patient leans forwards. The failure of the spine to move superiorly in a symmetrical manner indicates sacroiliac dysfunction |
| Contralateral Kemp’s test | Usually Kemp’s test (forced lateral flexion with extension) is used as a test for lumbar spine disorder and will produce ipsilateral pain; however, a sacroiliac syndrome will cause contralateral pain |
| Supported Adam’s test | Patients with a sacroiliac problem often report pain on slight forward flexion (5°–15°). If the sacrum is braced against the examiner’s thigh and the ilia held firmly, the patient can flex with reduced pain and trepidation |
| Digital palpation | If there is inflammation in the sacroiliac joint, palpation along its easily identified posterior margin will usually be painful |
Differential diagnosis

Figure 5.01 • The thigh thrust sacroiliac joint provocation test.
(Reproduced from Manual Therapy17 with permission.)
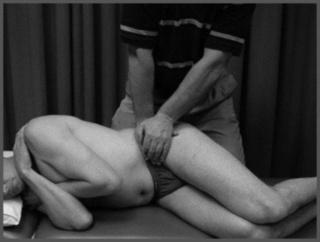
Figure 5.02 • The compression sacroiliac joint provocation test.
(Reproduced from Manual Therapy17 with permission.)
When it comes to the hip joint, the main aim of the differential diagnosis is to distinguish between intra-articular pathology, extra-articular pathology, and those conditions that can mimic hip pain. These are summarized in Table 5.02.3,21,22
Table 5.02 Causes of pain around the hip joint
| Intra-articular | Extra-articular | Mimickers |
|---|---|---|
The clinician should also be alert for paediatric cases presenting as knee pain without discernible cause. Two common hip conditions often present in this manner: slipped capital femoral epiphysis and Legg–Calvé–Perthes disease, and both have prognosis directly related to early detection.23
Technique and protocols
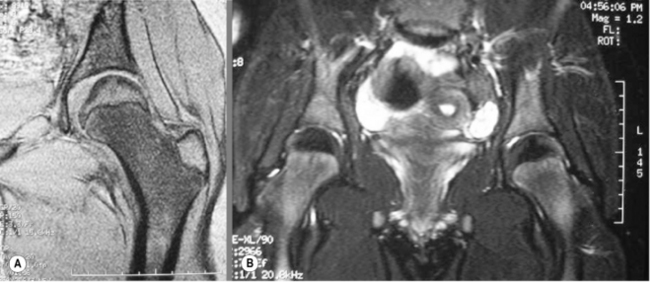
During any MR imaging evaluation, patient co-operation is critical. For evaluation of the hip, the patient should lie supine with mild internal rotation of the feet. Symmetry of rotation of both feet is important when both joints are examined simultaneously, which they often are to compare the appearance of the trochanters and adjacent muscles.24–26 Two types of images are available: a screening examination of both hips, or a higher-detail study of a single joint (Figure 5.03).
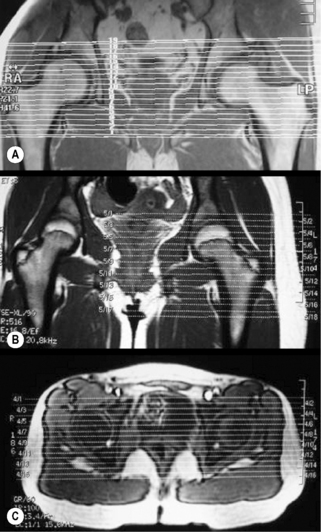
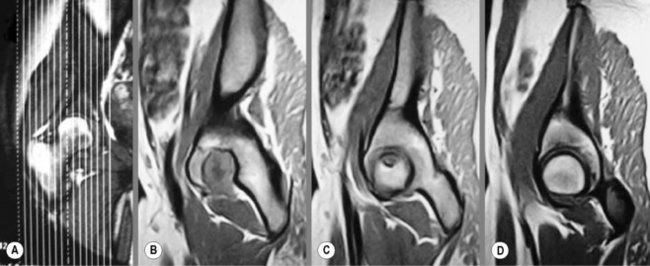
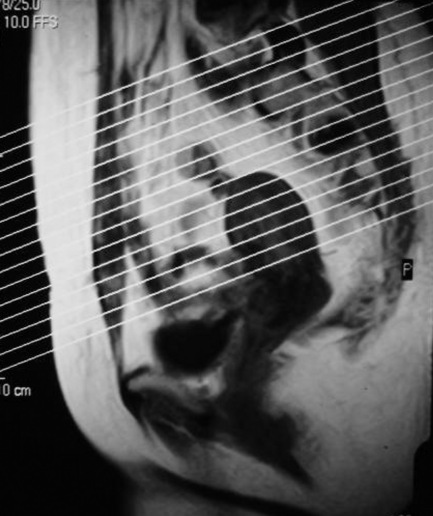
The study begins with a plan scan (or ‘scout’ view) through the level of the femoral head and will usually include axial and coronal views (Figure 5.04). T1-weighted and fluid-sensitive images will be obtained in multiple planes. Depending on the pathology suspected, sagittal views may also be acquired (Figure 5.05). Fat-suppression techniques are very commonly used in the hip and pelvis to show early changes in marrow signal.24,25,27,28
Intravenous contrast is not routinely utilized but may be helpful to differentiate cystic from solid masses or early ischaemic changes and in the evaluation of labral pathologies that have proven inconclusive on normal MR protocols. In these situations, findings may be accentuated even more if paired with fat-suppression techniques.25,27,29,30
Evaluation of the sacrum, sacroiliac joint and superior bony pelvis anatomy requires different positioning for the patient and should be ordered separately. The patient is often asked to lie supine with the knees slightly bent and hip joint mildly flexed; this position precludes good visualization of the iliofemoral joint. The planes of imaging for these areas is also different; in cases where sacroiliac arthropathy is suspected, images obtained in an oblique coronal plane parallel to the joint may be helpful (Figure 5.06). Intravenous administration of contrast can help identify early sacroiliitis. If pathology is suspected in the posterior soft tissues, imaging in the prone position may be also considered, to limit compression of the soft tissues.24,25,27,31,32
Normal anatomy and common variants
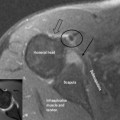
MR imaging displays osseous and soft tissue structures with great clarity; the osseous anatomy is best evaluated on the T1-weighted sequences. The acetabular fossa is a deep pocket that covers approximately 40% of the surface of the femoral head. The thick fibrocartilaginous labrum and transverse acetabular ligament completely encircle the acetabulum. Both structures will be demonstrated as low intensity areas on most of the MR sequences.33
The femoral head is generally spherical and covered by articular cartilage with the exception of the insertion point of the ligamentum teres: the fovea centralis. Covering the proximal femur is the articular capsule extending from the supra-acetabular region to the femoral neck.34,35 It is a normal finding to see a small amount of fluid inside the joint space (Figure 5.07). Adjacent to the capsule is one of the largest synovial bursae of the body: the iliopsoas bursa. It is seen as a high intensity area on fluid-sensitive images, sandwiched between the muscle and the capsule. In a small percentage of the population, it may even communicate with the joint.36



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


