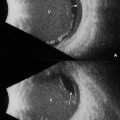
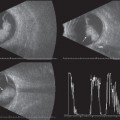
8 Aside from the clinical evidence of optic nerve disease based on findings ranging from afferent pupillary defect, decreased color vision, pale discs or disc swelling, the retrobulbar optic nerve is inaccessible for clinical evaluation. With the development of computed tomography (CT) and magnetic resonance imaging (MRI), visualization of this portion of the optic nerve is possible. But however sensitive these tests may be, there is still a wide variance in the differentiation of specific lesions involving the optic nerve. In particular, CT and MRI are less sensitive in distinguishing fluid beneath the nerve sheaths versus a solid mass lesion. Using contact B-scan, the echographer has the capability of evaluating the optic nerve from the disc to about two-thirds into the orbit. Performing axial scans is an excellent way to evaluate the intraocular portion of the nerve for disc elevation; however, it is not the best way to rule out optic disc drusen because there is usually significant sound attenuation from the lens, which may mask the appearance of drusen, especially if they are small. Both drusen and elevation can be imaged using a longitudinal approach, or with cross-sectional views. If drusen or disc elevation is present, it can be easily identified. In cross section, the retrobulbar nerve appears as a distinct, round, relatively low reflective structure. When there is fluid within the sheaths, an echolucent crescent shape can be imaged to the right of the round nerve proper. If solid thickening of the nerve is present, the borders may not be as distinct as the normal nerve, and if calcium is present within the sheaths, it can easily be detected. To image the nerve with the B-scan, the patient should be fixating in primary gaze. The probe is placed temporally and the back of the probe is rotated forward with the gain set at a medium level. Obtaining measurements of the retrobulbar optic nerve using the B-scan can be difficult, and it is not recommended, but the information obtained may be adequate for evaluation of children and non-cooperative patients. Standardized A-scan evaluation of the retrobulbar optic nerve has been shown to be an effective, accurate method for determining the diameter of the optic nerve and for detecting the presence of increased subarachnoid fluid (ISAF) or solid lesions involving the nerve. The A-scan probe is also placed temporally with the patient fixating in primary gaze. The gain should be set at the standard tissue sensitivity setting for the probe/machine combination. Because the optic nerve is a homogeneous structure, it will produce a low reflective defect within the normally high reflective echo pattern of the orbital tissue. Measurements should be taken from both the anterior and posterior portions of the nerve, as it is possible for a patient to have both a fluid and solid component to optic nerve thickening. Failure to evaluate the nerve completely could lead to misdiagnosis. The normal nerve measures from 2.3 to 3.3 mm in diameter from the inner aspects of the arachnoid sheaths. If the nerve measures larger than normal in primary gaze, a 30-degree test should be performed to determine if the increased thickness is due to fluid within the arachnoid sheaths or if it is secondary to a solid mass lesion. To perform this test, the patient should be instructed to look ~ 30 degrees toward the probe that is placed on the globe temporally. Measurements should then be repeated both anteriorly and posteriorly and compared with the measurements obtained in primary gaze. As the eye moves 30 degrees, if fluid is present, it will flow back along the nerve and the measurements obtained will be smaller (at least 10%) than the primary gaze measurements. If no fluid is present, the measurements in 30-degree gaze will remain similar to those obtained in primary gaze. In this case, the possibility of solid optic nerve thickening exists.
The Optic Nerve
♦ Optic Nerve Head Drusen
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


