
The Passive Navigational System: Application and Procedure for Use in the Operating Room
The world of image-guided neurosurgery is constantly changing and evolving. Several companies are marketing surgical navigation systems; each employs similar steps to bring usable image guidance into the operating room. These steps include preoperative imaging, surgical planning, surgical registration, intraoperative localization, and intraoperative navigation.1–2 Optically tracked systems are generally grouped into two categories with regard to the way in which they localize. The first group uses active localization. This group uses either light emitting diodes (LEDs) that flash, emitting light or ultrasonic wave pulses, which are triangulated by the camera.3 The second group uses passive optical navigation. In this group specially designed reference surfaces reflect light. The light source in the passive group usually comes from the camera or camera system and it bathes the entire field looking for reflections.1,4 This chapter describes the theory behind each step involved in the surgical navigational system and discusses an implementation procedure for the BrainLAB VectorVision neuronavigation system (BrainLAB USA, Redwood City, CA). The BrainLAB system uses a passive reference frame for image localization and navigation.5
 Description of Components
Description of Components
The BrainLAB VectorVision neuronavigation system is a frameless, intraoperative, image-guided, localization system. It consists of three main components: a computer planning station, an intraoperative localization camera, and an intraoperative computer display.5
The computer planning station, consisting of a docking station and a laptop, is the location of all the surgical planning. The docking station is the site of network connection and allows for an initial site for image transfer and a constant battery supply. The laptop is an Intel Pentium III processor running Windows NT.5
The intraoperative localization camera and intraoperative computer display make up the single VectorVision intraoperative, image-guided navigation system (Fig. 7–1). Both the camera and the computer screen are mounted to individual arms that allow for flexible positioning in the operating room. The camera system consists of two infrared emitting cameras arranged at a fixed distance of 48 cm apart. The camera works by passively detecting reflections of infrared flashes. The infrared flashes are reflected by passive marker spheres that are located in a fixed orientation in relation to the patient’s head. The spheres are 8 mm in diameter. The markers must be gas-sterilized and can be reused as long as the reflective covering is intact. The spheres are simply screwed onto different adapters that are used in the field.1,5
 Fiducial Placement
Fiducial Placement
Proper fiducial placement can greatly increase the registration accuracy in the operating room. For the patient to be registered during surgery at least four fiducial markers must be visible by the camera.5 Therefore it is useful to know where the surgeon is planning to make the incision and to localize the fiducial markers where they are most likely to be visible in the operating room.
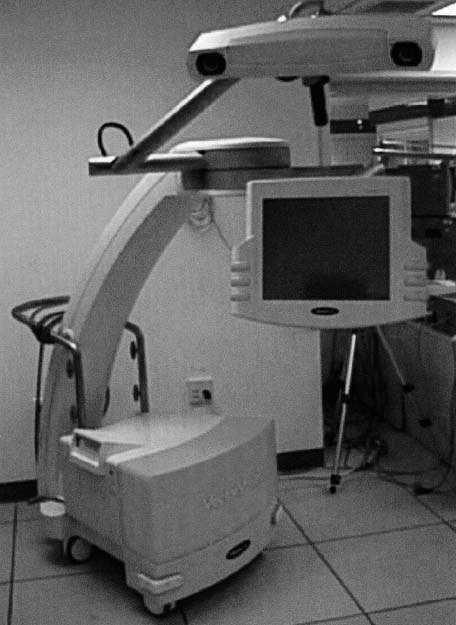
FIGURE 7–1. BrainLAB VectorVision Navigation System (Redwood City, CA). This device is the interface between the image transfer and planning process and the operating room. The computer is housed in the base of the machine, which is also the point of zip disk insertion and processing. As shown in the image, both the touch screen interface and camera are on separate adjustable arms that allow for the greatest mobility in the operating room. The touch screen can be used nonsterile by a circulator or technician or can be made sterile with the use of a specially designed plastic drape. This feature allows the surgeon to use image guidance without assistance.
We have found it is best to use at least six fiducial markers per patient. Less than five or six markers provide reduced registration accuracy. Skin fiducial markers are by nature more mobile than bone implanted markers. For this reason it is important to place markers in locations where the skin is least likely to be deformed or shifted during scanning. Accuracy can be greatly improved by localizing fiducials around the midline and away from muscles.6 In a general case the fiducials are spread out over the head, placing two on the forehead, two straddling the midline near the top of the head, and two behind the ears, but avoiding any muscular tissue of the mastoid.
Patient positioning is also important to keep in mind. Not only can it be difficult to see the fiducial markers, but also registration accuracy can change with positioning of the head. If the patient is scanned supine and the case is going to be performed in the prone position the surgeon risks a greater error in registration due to the normal shifting of the brain in response to gravity.6–7
 Image Acquisition
Image Acquisition
There are several ways in which images can be used in the operating room. At least one set of images must be used as the registration image. The images can be registered using the standard registration system (fiducial markers), landmark registration, or Z-touch (BrainLAB USA, Redwood City, CA) registration (Fig. 7–2). The fiducial registration system uses 5 to 6 marker sockets attached to the surface of the head. These markers must be on and visible during the scanning process and must remain in the same location until the patient is ready for surgery. Neither the landmark or Z-touch registration systems require patient preparation prior to the operating room. The landmark registration system recognizes user-defined landmarks on the patient to register the images in the operating room. Z-touch uses an infrared laser beam that scans across the structures of the face acquiring reference points that are used by the system for calibration.5

FIGURE 7–2. Z-touch registration instrument (BrainLAB, Redwood City, CA). This instrument can be used to register a patient in the operating room to images that do not have fiducial registration markers. The red laser beam emits an infrared beam of light that can be seen by the camera when the button (shown here) is pushed all the way down. This beam of light traces the structural features of the face, primarily picking out the bridge of the nose and the structures around the eye.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


