Shoulder Checklists
 1
1
Radiographic examination
AP external rotation
AP internal rotation
Axillary view
Y-view
Grashey (posterior oblique) view
 2
2
Common sites of injury in adults
Fractures
Midshaft of clavicle
Avulsion of the greater tuberosity of the humerus
Surgical neck of the humerus
Dislocations
Acromioclavicular joint dislocation
Dislocation of the glenohumeral joint
Anterior dislocation
Posterior dislocation
Luxatio erecti
 3
3
Common sites of injury in children and adolescents
Greenstick fracture midshaft of clavicle
Acromioclavicular joint dislocation
Epiphyseal separation proximal humerus
Pathologic fracture of unicameral bone cyst (UBC) of proximal humerus
 4
4
Injuries likely to be missed
Posterior dislocation of the shoulder (glenohumeral) joint
Injuries in and about the sternoclavicular joint
Sternoclavicular dislocations
Fractures of the medial clavicle
 5
5
Where to look when you see nothing at all
Check again for findings to suggest a posterior dislocation of the glenohumeral joint.
Is the joint space widened?
Is the humeral head fixed in internal rotation?
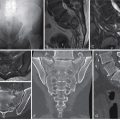
Look closely at the rim of the glenoid fossa, particularly the anterior rim, on the AP view.
Is the ovoid rim intact?
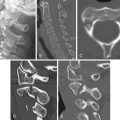
Look for a subtle, nondisplaced fracture of the mid-clavicle.
Need clear view of the mid-clavicle, free of the underlying ribs and scapula.
AP view with 15° of cephalic angulation may be required to disclose the fracture.
Shoulder – the Primer
 1
1
Radiographic examination
AP external rotation
AP internal rotation
Axillary view
Y-view
Grashey (posterior oblique) view
The standard radiographic examination of the traumatized shoulder should include at least three of the five standard views listed above. These have been selected because they have proven to disclose the majority of fractures and dislocations. My personal preferences are the four illustrated ( Figure 2-1 ). Two AP views should be obtained, one with the humerus in external rotation and the second with the humerus in internal rotation ( Figure 2-1 A , B ). The Grashey or posterior oblique view ( Figure 2-1 C ) is a tangential view of the glenohumeral joint obtained with 35° posterior rotation of the shoulder. This view is particularly useful in disclosing fractures of the anterior glenoid rim and confirming the presence of a posterior (glenohumeral) shoulder dislocation as identified by an overlap of the humeral head and glenoid in this projection.

The axillary view ( Figure 2-1 D ) also depicts the glenohumeral joint and margins of the glenoid to good advantage and therefore is useful in identifying glenoid rim and coracoid fractures as well as dislocations of the glenohumeral joint.
 2
2
Common sites of injury in adults
Fractures
Midshaft of clavicle
Avulsion of the greater tuberosity of the humerus
Surgical neck of the humerus
Dislocations
Acromioclavicular joint dislocation
Dislocations of the glenohumeral joint
Anterior dislocation
Posterior dislocation
Pattern of search
Diagrams of the shoulder ( Figure 2-2 ) pinpoint the common sites of fracture and dislocation in adults. The most common sites of fracture are identified by broad red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites.

Clavicle fractures
Eighty plus percent of fractures occur in the midshaft. They may be nondisplaced ( Figure 2-3 A ) or displaced and comminuted, commonly with elevation of the medial fragment ( Figure 2-3 B ). Fractures of the outer third may involve the AC joint and disrupt the coracoclavicular ligament. Fractures of the medial third are uncommon.

Acromioclavicular dislocations
In the normal AC joint the inferior cortex of the outer end of the clavicle aligns with the under-surface of the acromion ( Figures 2-4 A ). The width of the normal AC joint is 4 to 6 mm. The normal distance between the superior tip of the coracoid process and inferior surface of the adjacent clavicle is approximately 1.2 cm. Disruption of the coracoclavicular ligaments results in an increase in this distance.

Acromioclavicular dislocations vary from a simple sprain manifest by widening of the AC joint, to disruption of the joint with slight elevation of the clavicle with intact coracoclavicular ligaments ( Figure 2-4 B ), to complete disruption of the joint with elevation of the outer end of the clavicle and tears of the coracoclavicular ligaments increasing the coraclavicular distance ( Figure 2-4 C ).
Acromioclavicular dislocations may require weight-bearing views to disclose the true extent or even the presence or absence of injury. Weight-bearing views are not required if the outer clavicle is elevated and the coracoclavicular distance is increased above 1.2 cm. In any other circumstance with a clinical suspicion of AC joint injury, weight-bearing views should be obtained to determine the full extent of the injury.
Rockwood classification of AC joint dislocations ( Figure 2-5 )
Type I consists of a sprain of the ligaments about the joint. There is no displacement of the clavicle or widening of the joint. The radiographic findings are normal. Type II is a subluxation of the AC joint. The outer end of the clavicle is slightly elevated in relation to the acromion, and the AC joint may be widened, but the clavicular ligaments remain intact, and the coracoclavicular distance is normal. In Type III the coracoclavicular ligaments are disrupted, and the distance between the clavicle and coracoid is increased >1.2 cm. The clavicle is elevated. Type IV is a posterior dislocation of the clavicle. The outer end of the clavicle pierces into or through the trapezius muscle. The clavicle may be elevated or, at times, depressed. Posterior displacement can be seen on the axillary or Y views. In Type V the clavicle is markedly elevated and lies subcutaneously. The clavicle is at least partially detached from its muscle attachments. Type VI is an inferior dislocation wherein the outer end of the clavicle comes to rest beneath the coracoid process posterior to the coracobrachialis tendon.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


