11 The temporomandibular articulation
Introduction
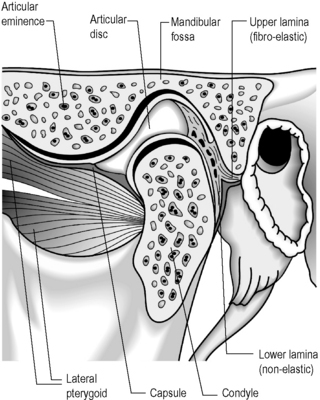
The temporomandibular articulation (TMA) is formed between the ovoid mandibular condyle and its complementary elliptical articulating surface on the glenoid fossa of the temporal bone (Figure 11.01).1,2 Although a true synovial joint, it eludes traditional classification and different authors will place it in different groups.
Many simpler texts will term it a hinge joint (ginglymus)3; however, this overlooks the gliding phase of movement, typical of arthrodial joints – for this reason, some authors classify the joint in a unique category, terming it ginglymoarthrodial.4 Although this describes the joint from a functional standpoint, structurally it is more commonly classified as a bicondylar joint; that is an ellipsoidal (or condylar) joint – one in which an ovoid head of one bone moves in an elliptical cavity of another (permitting all movements except axial rotation) with the additional feature of a meniscus between the articular surfaces. This feature also defines it as a complex joint.5–7
Regardless of the semantics over the joint’s classification (it is most probably easiest to regard it as unique; there is no directly comparable joint), the important thing for the clinician to understand is that it is composed of a series of complicated, interrelated osseous and soft tissue structures, each of which may be implicated in clinical syndromes. As such, the joint can be responsible for a significant level of morbidity with local symptoms including pain, restriction, stiffness, crepitus and clicking.8 It can also be responsible for referred pain syndromes and is an often overlooked cause of headache9–11; facial pain12,13; vertigo, tinnitus and ear symptoms14–18; and interrelated dysfunction elsewhere in the stomatognathic system (the dentition, mandible, cranium, spine and pelvis).19–21
The osseous structures centre around the articulating surfaces and the adjacent coronoid process; the soft tissue elements include the articular disc and its various attachments, a multitude of delicate ligaments, muscular insertion points and synovial and capsular components.2,3 There is considerable dispute about the contribution of these various elements to the symptoms of temporomandibular disorder (TMD),8 and diagnosis always needs to be carefully correlated with history and clinical findings; however, magnetic resonance (MR) imaging offers the clinician the chance to evaluate the articular disc in great detail. It is essential, therefore, to be able to differentiate the well-documented physiological, age-related changes from pathological conditions, which include internal derangement, tears, abnormal displacement (with or without reduction), dislocation and perforation. These, in turn, must be differentiated from internal signal abnormalities.22
History and examination
Because of the sequelae to and comorbidity with TMD, it is important to elicit a basic dental history from all patients. This should cover several key points (Box 11.01).23,24 As with any clinical history, it is also necessary to undertake a systems review and to explore psychological history, which is particularly pertinent in chronic cases.24,25
Box 11.01 The key points in eliciting a basic dental history from patients with temporomandibular disorder
Owing to the interrelated complexity of head and face pain disorders, it is necessary to evaluate non-masticatory structures in order to properly establish a differential diagnosis. This screening should comprise examination of the eyes, ears, cervical spine and cranial nerves.26–28
The examination of the temporomandibular joint should cover the muscles of mastication, the joint itself and the teeth.24 Whereas this last is more properly the province of the dentist or orthodontist, it is perfectly simple for any competent clinician to note the absence or significant decay of teeth, excessive wear or obvious malocclusion – all of which can be primary causative factors in TMD29–33 – and, if necessary, refer for an expert opinion and reconstructional or orthodontic intervention.
The examination of myofascial structures should start with observation of facial symmetry and evidence of muscle atrophy. Digital palpation should then be used to elicit the presence of myofascial trigger points in the muscles of mastication – temporalis, masseter and the medial and lateral pterygoids – plus associated muscles, including the digastric, suprahyoid, sternocleidomastoid and the intrinsic and extrinsic muscles of the cervical spine.34
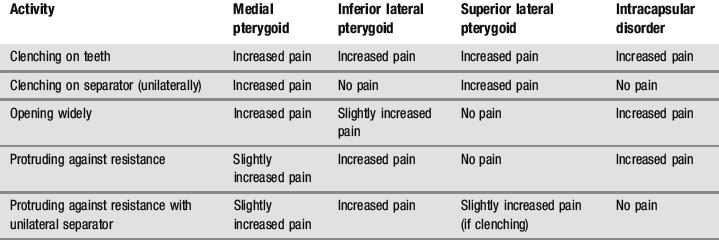
Because the pterygoids can be hard to palpate, functional manipulation can be used to assess these muscles. This is accomplished by contracting the muscles by clenching, both against the opposing teeth and a separator, and by protruding against resistance and then stretching by passive and active opening of the mouth. An increase in pain is regarded as a positive finding, although this needs to be carefully differentiated from intracapsular pain and restriction (Table 11.01).24,35
When evaluating temporomandibular gait, any lateral deviation on opening and closing should be noted, as well as the smoothness of transition from swing to glide phases. Trismus (popping, clicking or grating sounds from within the joint) can often be felt more easily than heard if the fingers are placed lightly over the joints during gait; alternatively, a stethoscope may be used. When the mouth is fully open, the maximum interincisal distance should be between 53 and 58 mm in an adult, equivalent to the width of the middle three fingers.36–39
Differential diagnosis
Temporomandibular disorders need to be differentiated from other facial pain syndromes, including: osseous disease; dental conditions; salivary and lymphatic disorders; neuropathic pain and headache; and miscellaneous conditions such as atypical facial pain.40 This is usually easy to achieve by competent history-taking and examination without recourse to diagnostic imaging.8
The different aetiologies of TMD also need to be differentiated, as the underlying cause will obviously affect both management and prognosis. The classification of TMD is detailed in Box 11.02; diagnostic imaging is of particular use in differentiating types II and IV TMD.8
Clinical indications for diagnostic imaging
Temporomandibular disorders can be classified as extra-articular or intra-articular, or can of course be a combination of both. Extra-articular causes of TMD are usually muscular in origin and are a common clinical entity presenting to a wide variety of primary healthcare practitioners. Aetiological factors include bruxism, often exacerbated by stress or anxiety, trauma, and occlusal disruption.41
The intra-articular causes of temporomandibular disorders, also known as arthrogenous TMD, are most commonly attributed to abnormalities affecting the meniscus: displacement, either temporary or chronic, degenerative joint disease, inflammatory disorders such as rheumatoid arthritis, infection or, rarely, tumour processes.8,42,43 Discal pathology is where MR imaging may be most useful, to determine the resting position of the meniscus and assess its movement during temporomandibular gait.44 Some meniscal dysfunction is also related to myopathology; for example, anterior disc displacement in the closed position, which reduces with opening, has been linked with a lateral pterygoid spasm, evidence of which may be detectable with MR imaging.45,46
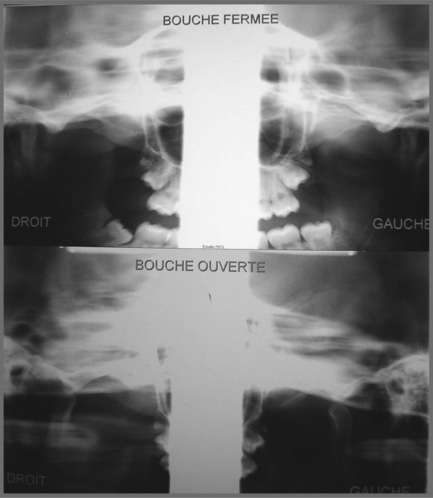
In former years, imaging of the TMA consisted of routine radiography, including the panoramic views which can provide some information regarding the shape, size and general state of the mandibular condyles (Figure 11.02); conventional tomography was also used to assess the open and closed mouth (Figure 11.03).47 High-resolution ultrasound may also be sensitive enough to detect gross internal derangement affecting the TM joint.48–50 Although computed tomography (CT) has also provided detail regarding the bony parameters of the TMA, MR imaging excels in the evaluation of the soft tissue components of the TMA, so often the origin of the patient’s complaint.49,51,52 Current knowledge of TMA pathologies has largely relied on both the clinical presentations of a range of conditions as well as the use of basic, invasive and not always helpful imaging modalities. With the advent of MR imaging, the understanding of the osseous component of articulations has been furthered and the soft tissues in and about the articulation have also moved firmly into the spotlight.22,47,49

Figure 11.02 • Panoramic digital imaging of the mandible illustrating the typical appearance of this image.
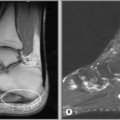
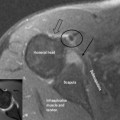
The distinct advantage of MR imaging and MR arthrography is that they allow for the excellent visualization of both bony and soft tissue anatomy using a technique that is only minimally invasive (Figures 11.04, 11.05). The advancement of the technology of imaging has led to significant improvement in the understanding of the complex nature of the anatomy and hence the pathology encountered in the TMA.53–55
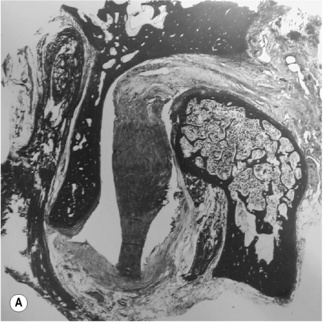
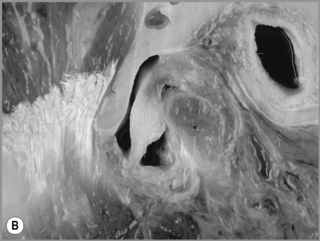
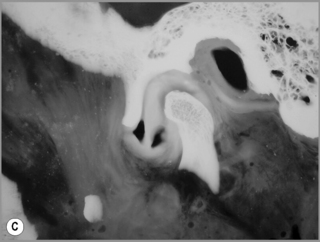

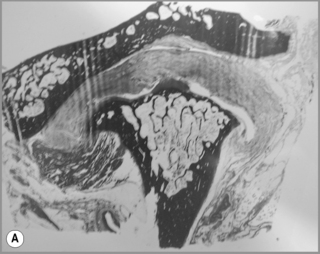
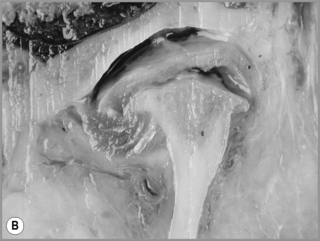

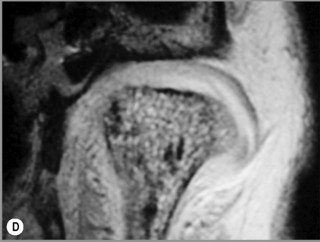
Figure 11.05 • Images of the same male cadaver as Figure 11.04. (A) Coronal slice through the right TMA at a microscopic level (right is lateral). Note the irregularities of the mandibular condyle, which represents a normal variation of the condylar surface, not usually appreciated on plain radiographs but which can be appreciated on special imaging. (B) The same specimen seen with the naked eye, allowing appreciation of the relationship between the previous image and the gross anatomy. (C) Faxitron image (radiograph) performed in the AP view demonstrating the relationship between the meniscus, mandibular condyle and the glenoid fossa of the temporal bone. (D) MR T1-weighted arthrogram showing how the meniscus is draped over the mandibular condyle, which is somewhat irregular.
Protocol
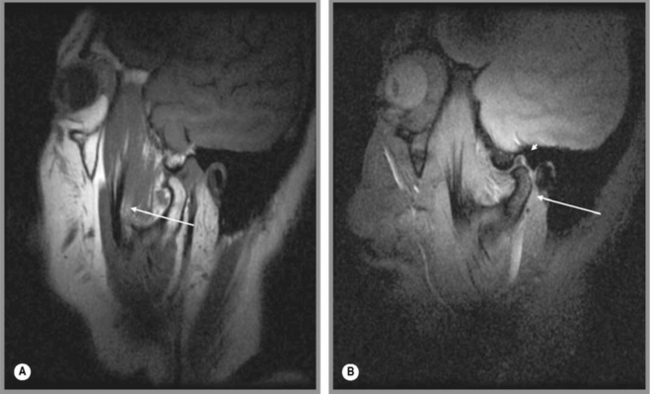
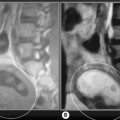
Normally, the patient is imaged in the axial plane to determine the orientation of the anterior condyles. From this, the sagittal oblique sequences are planned, with the slices perpendicular to this line, in both the closed- and then the open-mouth position (Figures 11.06, 11.07), noting in particular the location of the meniscus in both positions. Coronal oblique images may also be performed and are planned off the initial axial sequence along the long axis of the condyles. Both T1-weighted and T2-weighted images may be performed, in both the closed- and open-mouth positions, depending on the preference of the imaging centre and based on the type of MR machine.56–58
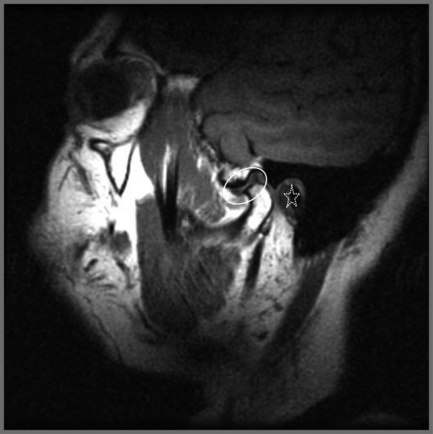
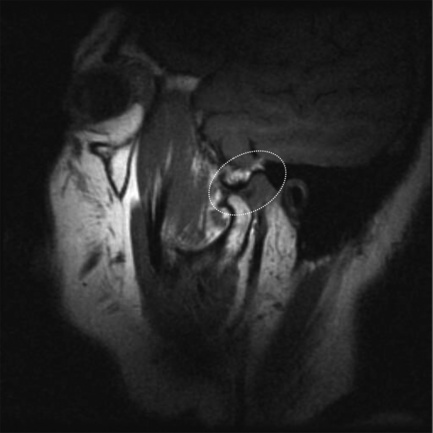
Figure 11.07 • Sagittal oblique, T1-weighted image of a normal temporomandibular articulation in the open-mouth position. Note the altered position of the mandibular condyle with respect to the glenoid fossa of the temporal bone (Figure 11.02). Anterior translation of the mandibular condyle has occurred, with an alteration of the relationship with the meniscus (oval).
Normal imaging anatomy
Osseous structures
Normally, on the sagittal image, the condyles should be oval in shape and covered by a thin layer of cortical bone (Figure 11.08), which on the MR image will appear with low signal intensity. The signal intensity should be homogeneous and, on the fluid-sensitive sequences, should be intermediate to low signal. On the T1-weighted sequence, the signal intensity should be brighter than on T2-weighting and be the same as that in the remaining normal bone marrow visualized elsewhere on the image (Figure 11.09).

Figure 11.08 • A sagittal section of the temporomandibular joint demonstrating the location, shape and relations of the articular disc.
Reproduced, with permission, from Gray’s Anatomy 39e, Standring S, ed, (Elsevier, 2005)
Articular disc
The articular disc is a lozenge or elongated oval shape and has a superior and inferior surface. The superior surface is concavo-convex from anterior to posterior to conform to the contours of the articular fossa and condyle. The inferior surface is moulded to the condyle of the mandible and is, therefore, concave (Figure 11.08).1,59 The disc completely divides the TMA into two distinct compartments – superior and inferior, both of which are usually compressed – and, ordinarily, there is no interconnection; however, in the older population there can be a significant degree of degeneration in the region of the disc. This may result in partial or complete perforation of the disc, thus allowing communication between the superior and inferior joint spaces.2,60,61
The disc is attached both to the fibrous capsule and to the lateral pterygoid muscle anteriorly. There are extensions that pass medial and laterally, which head towards and insert into the mandibular condyle. The posterior portion of the disc divides into superior and inferior portions, or lamellae. The upper, or superior, lamella inserts into the posterior margin of the mandibular fossa and is composed of fibroelastic tissue. The lower, or inferior, lamella is attached to the posterior condyle but is not elastic and is composed of white fibres.53
The thickest portion of the disc is just posterior to the central portion at a position that corresponds with the deepest part of the mandibular fossa. The disc has been further divided into various parts according to the anatomical appearance – anterior extension, anterior band, intermediate zone, posterior band and the bilaminar zone (upper and lower lamellae).1
Morphological evaluation of the superior and inferior surface of the disc reveals some distinct differences in the nature of pathological changes. The inferior surface is by far the more commonly affected in patients, though without discal symptoms, suggesting that there may be no correlation between the presence or absence of disc derangement and the degree of change to disc morphology. Although the exact function and related biomechanical properties of the disc have not been fully determined clearly, the highly ordered crimped nature of the collagen indicates its viscoelastic ability to be loaded, and to become stiffer with time.62,63 There is also a change in the properties of the collagen of the disc with time; it becomes stiffer.63 This loss of proteoglycans and increased water content probably makes the disc more susceptible to mechanical stresses and increases the risk of disc disruption.
On the microscopic level, fibres extend from anterior to posterior and also in the vertical direction. The chief component of the disc is the glycosaminoglycan chondroitin sulphate. There is a direct relationship between the disc morphology with respect to its length and degree of displacement. As the degree of displacement increases, so the convexity of the posterior slope of the articular eminence decreases. As the disc displacement increases, so do the inferior, superior and posterior joint spaces.64
The meniscus of the TMA is visible in all planes on MR imaging: sagittal oblique, axial and coronal oblique. The appearance of a normal meniscus is that of a biconcave structure of low signal intensity covering the mandibular condyle (Figures 11.04, 11.05). The signal intensity within the meniscus is usually homogeneous, although this depends somewhat on the age of the patient; in the older patient, small alterations in intrameniscal signal intensity may be considered normal.
In the sagittal oblique plane, the meniscus should be directly superior to the mandibular condyle in the closed-mouth position. On the T2-weighted (fluid-sensitive) sequences, the meniscus is outlined by the fluid located in the superior and inferior compartments; this is particularly pronounced on the sagittal oblique slices (Figure 11.09). There is neither means to quantify the volume of fluid that is considered normal or abnormal nor agreement as to what defines these terms; indeed, some authors consider that any fluid noted on the fluid-sensitive sequences should be considered evidence of a joint effusion. The assessment is, therefore, largely down to the experience of the individual radiologist.30,65–69



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


