3 The thoracic spine
Introduction
Perhaps more than any other area, pain in the thoracic spine and its associated rib articulations requires differentiation from referred visceral pain and pathology, which can easily mimic musculoskeletal problems.1 However, the thoracic spine is one of the most difficult areas to image with plain film radiography. On an x-ray, the thoracic cage is superimposed over the vertebral bodies; the discrepancy in tissue density between the osseous thoracic spine and the lung parenchyma creates a confluence of densities that precludes the acquisition of high-quality radiographic images.2 This is particularly true for the lower thoracic spine, owing to the superimposition of the diaphragm, and the upper regions of the thoracic spine, owing to the soft tissues of the shoulder.
Cross-sectional imaging of the spine, spinal cord and surrounding anatomical structures has therefore contributed substantially to the detection and characterization of disorders affecting the thoracic spine; however, magnetic resonance (MR) imaging of this area is not without its own complications, which mainly arise from motion artifacts. Image quality can be affected by the pulsation of the heart, the respiratory cycle, and the vertical pulsatile movement of the blood and the cerebrospinal fluid through the thoracic region (Figure 3.01).3 It is therefore important to recognize that the method of imaging the thoracic spine has been designed to reduce the effect of motion artifacts by utilizing techniques such as peripheral gating or saturation pulses.4,5
MR imaging of the thoracic spine is often performed to determine the presence of a disc lesion. Although such lesions tend to be less common and also smaller in volume than those in other spinal areas, because the dimension of the thoracic spinal canal is relatively smaller, the risk of neurological compression is correspondingly higher.6,7
MR imaging has superior imaging quality of epidural and bone marrow involvement compared to other general imaging modalities, providing a means for the differentiation of normal haematopoietic marrow from infiltrative processes such as metastatic disease. MR imaging, by virtue of the differing signal intensities, allows for the diagnosis and evaluation of disorders affecting the epidural fat, spinal cord, subarachnoid and intramedullary regions.8
By contrast, CT provides beautiful detail of bony structures but is somewhat limited in its depiction of canal lesions. MR imaging also allows the depiction of the soft tissue structures around the spine, including paraspinal soft tissue and neural structures; this is useful in conditions such as paraspinal abscess formation and neural tumours.9,10
History, examination, diagnosis and indications for imaging
Examination of the thoracic spine is considerably more difficult than that of the cervical and lumbar areas. There is a dearth of orthopaedic tests of diagnostic significance; the dermatomes overlap to the point whereby a single root lesion remains occult; there are no reliable myotomal indicators and no deep tendon reflexes, although the umbilical reflexes can sometimes indicate a radicular lesion and long tract signs can also be an important indicator of central cord pathology.6,11
This makes the history even more important: apart from a thorough review of the cardiovascular and respiratory systems, the thoracic spine also contains the sympathetic trunk and so a generalized screen of the patient’s systemic health is also essential.12,13
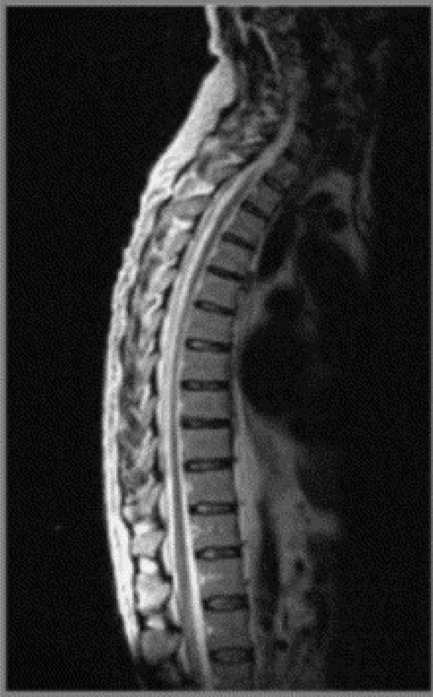
Observation of the patient can provide important clues. Scoliosis is a condition that commonly affects the thoracic spine, and which is easily seen.14 Hyperkyphosis can also be associated with Scheuermann’s disease (juvenile discogenic disease), ankylosing spondylitis and compression fractures, most commonly secondarily to osteoporosis; the age and sex of the patient is therefore important in indicating the differential diagnosis (Figure 3.02).15

Palpation can also be suggestive of conditions such as thoracic facet injury, costovertebral syndrome and costochondritis (Tietze’s syndrome), all common causes of thoracic pain; however, because of the difficulty involved in definitive testing, diagnostic imaging is all the more important.16,17
Protocol
MR imaging of the thoracic spine requires the patient to lie supine during the examination; usually the patient enters the magnet headfirst. The complete MR examination lasts approximately 30–45 minutes, depending on the sequences required. It is, however, possible for patients to move between the various sequences, each of which commonly lasts for around 2 to 3 minutes. A spinal coil is placed under the patient to increase the quality of the image and a triangular foam pad is frequently placed under the knees, which may affect the normal spinal curvature. A positioning light is centred over the sternum in the midline.4,5
The field of view in MR images of the thoracic spine is approximately 16 cm in the sagittal plane and 14 cm in the axial plane. Slice thickness is usually 3–4 mm.4,5 The initial sequence is the coronal localizer (scout view); this is taken to verify the patient positioning and ordinarily includes C2 in order to correctly identify the thoracic levels. Imaging slices may be acquired either from the left to right field borders or from right to left of the vertebral bodies and it is important to verify this by noting the order of the slice numbers on the localizer view.
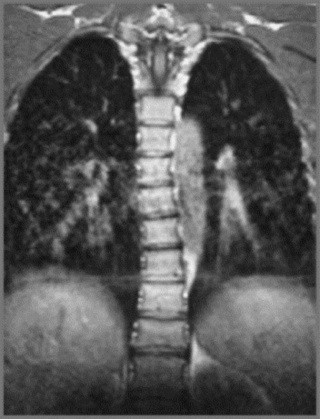
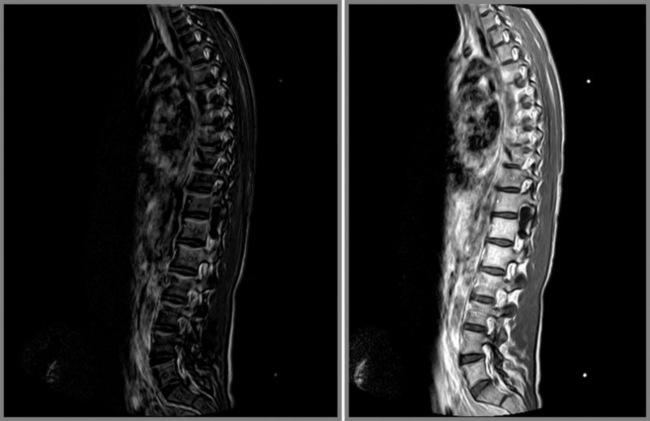
MR imaging of the thoracic spine commonly consists of T1-weighted and fast spin echo (FSE) T2-weighted sequences in the sagittal plane (Figures 3.03, 3.04). In the axial/axial oblique plane, T2-weighted FSE (or intermediate weighted axial FSE) images parallel to the disc are acquired (Figure 3.01). The oblique plane is very useful to acquire information at the level of the intervertebral disc and in cases of scoliosis; the coronal/frontal plane may also be included, again particularly in scoliotic patients (Figure 3.05).


Specific protocols may be used in particular clinical circumstances. Most MR imaging thoracic spine protocols for metastases include T1- and T2-weighted sagittal and axial images with repetition of the T1-weighted images following the addition of gadolinium.18 Alternative imaging sequences may include short tau inversion recovery (STIR) and fat suppression. The use of STIR is especially useful in increasing the sensitivity of lesion detection in the posterior elements of the vertebrae.19
Normal anatomy and variants
Intervertebral disc
The thoracic intervertebral disc is important to evaluate owing to the relatively smaller spinal canal diameter in this area of the spine, which predisposes to a higher risk of neurological involvement in thoracic disc herniations.7 The hydrated nucleus of the normal intervertebral disc should be appreciated, together with its relationship to the cerebrospinal fluid of the anterior subarachnoid space. In degenerative disc disease, a reduction in hydration is demonstrated as hypointensity in the disc on T2-weighted sequences.20
Symptomatic thoracic disc lesions, such as extrusions, are uncommon, and present a particular diagnostic challenge to the clinician.21 Sagittal, T2-weighted FSE sequences are excellent for displaying indentation of the ventral thecal sac and effacement of the spinal cord by a thoracic disc extrusion. Axial images help delineate lateralization of the disc lesion and evaluate impingement of the traversing nerve roots.
Because of the relatively smaller size of thoracic discs, they may appear hypointense on T2-weighted sequences compared to discs in other areas of the spine (Figures 3.03B, 3.04).
Vertebral body
The individual osseous components of the vertebral bodies are evaluated well using MR imaging; this is particularly true of the bone marrow. Cortical bone should appear as low signal intensity owing to the lack of mobile protons, especially on T1-weighted images (Figure 3.06). There should be no evidence of change in the contour of the vertebral bodies, which should have a homogeneous signal intensity on T1-weighted sequences (Figure 3.07).22 Because of the higher fat content of the marrow, the vertebral body will be of intermediate or higher signal intensity relative to the adjacent disc.


The normal appearance of the vertebral body on T2-weighted sequences is that of homogeneous low signal intensity when compared with that of the intervertebral discs and cerebrospinal fluid (Figure 3.08).
A variation of the normal MR imaging appearance of bone marrow may include the presence of small foci of high signal (relative to the surrounding bone marrow) on T1-weighted imaging, which reduces on the T2-weighted sequences. This most likely represents an intraosseous lipomatous deposit, a normal variation.4,5
Another common phenomenon is high signal intensity in the bone marrow on both T1-weighted and T2-weighted sequences, representative of an intraosseous haemangioma. This condition does not usually have clinical consequences for the patient and is almost invariably an incidental finding. In less than 1% of patients, haemangiomas may become symptomatic – particularly if they begin to expand, and the expansion is posterior. Such expansion is determined by evaluating the posterior wall of the vertebral body for evidence of slight posterior bulging of the cortical margin; this may suggest the presence of expansion before there is frank clinical evidence.23,24
By contrast, if high signal intensity is evident in the bone marrow on T2-weighted sequences and decreased signal intensity on T1-weighted sequences, this should be a cause for concern, since this pattern is suggestive of an infiltrative process such as metastatic disease, and should be followed with more specific sequences such as STIR or out-of-phase GRE MR imaging, and T1-weighted images with the addition of gadolinium.4
Spinal cord
The spinal cord should appear as intermediate (grey) signal intensity on all pulse sequences (Figure 3.09), although on T2-weighted sequences it may be possible to distinguish the white and grey matter of the spinal cord. The spinal cord should be evaluated for shape, size, symmetry and internal organization to exclude the presence of disorders such as spinal cord impingement or syrinx formation.

The anterior, lateral and posterior columns (white matter) are demonstrated as hypointense signal intensity on the T2-weighted sequences. The cerebrospinal fluid is visible on MR imaging, visualized well on T2-weighted sequences as hyperintense signal and on T1-weighted sequences as hypointense signal, compared to the bone marrow signal intensity.5
Intervertebral foramen
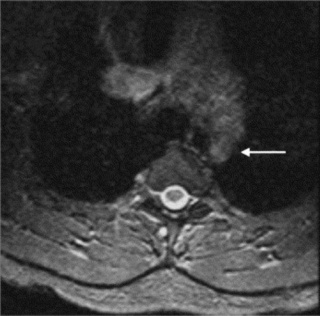
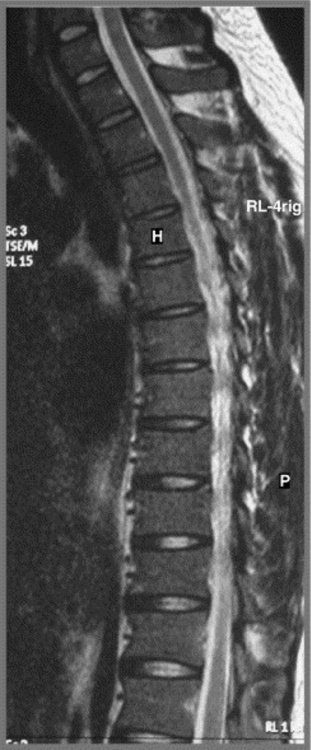
MR imaging allows for definition of the size and morphology of the intervertebral foramen as well as its contents. The thoracic foramina are best visualized on the axial and sagittal sequences (Figure 3.10). Identification of the exiting nerve roots surrounded by their perineural fat may be possible. Disorders that can involve the IVF in the thoracic spine include nerve root tumours, such as neurinomas, or abnormalities affecting the nerve root sleeve such as meningocoele or diverticulum formation (Figure 3.11).25

Pathological conditions
Thoracic disc lesions
The articulations with the ribcage make the thoracic spine the least mobile of the spinal regions; injuries to the thoracic spine and intervertebral discs are, therefore, less common than to the adjacent cervical and lumbar regions. There are, however, some factors that may predispose individual patients to disc lesions in the thoracic spine. Owing to the thoracic kyphosis, the spinal cord lies anteriorly in the spinal canal, approximating to the posterior longitudinal ligament and providing a greater propensity for ventral cord compression.26 The thoracic spinal canal is also smaller than its cervical and lumbar counterparts and, although the spinal cord too is less massive, the size relative to the canal is still greater than in other areas of the spine. The clinical consequences of this are that although thoracic disc lesions may be less common, there is a higher chance of them being symptomatic, as the neural structures are more prone to compressive or irritative pathology.13
Though not a common entity, thoracic disc lesions are, nevertheless, considerably less rare than once thought. Due to the paucity of associated clinical findings, thoracic disc lesions were difficult to diagnose before the advent of MR imaging and they were once thought to represent fewer than 5% of all disc lesions.21 The incidence of symptomatic thoracic disc lesions is still thought to be low (although this is difficult to ascertain and there is often no way to accurately determine whether a patient’s symptoms relate to discal pathology by clinical examination alone), whilst the presence of asymptomatic thoracic disc lesions may be as high as 37%21



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


