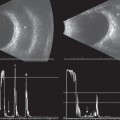
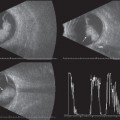
3 The normal, clear vitreous appears black or acoustically empty on B-scan and as a flat baseline on standardized A-scan. Vitreous floaters occur normally as a result of aging and appear as white dots within the normally black vitreous cavity. These opacities can be very mild, such as a single floater that may go unnoticed and not affect visual acuity, or they may be extremely dense, affecting the patient’s perception of visual function. As a general rule, opacities within the vitreous look similar no matter what their origin; therefore, the clinical history is an important component when reporting the echographic findings following an ultrasound examination. For instance, if on initial clinical presentation a patient has an anterior chamber hyphema, the presence of opacities in the vitreous on ultrasound are more likely to represent hemorrhage. However, if a patient has a dense cataract clinically with no view of the posterior segment and opacities are noted within the vitreous cavity echographically, it is not possible to differentiate the nature of the opacities. Asteroid hyalosis is a clinical finding that displays a classic echographic appearance. Highly reflective signals that move separately from each other are noted within the vitreous cavity. Typically, vitreous opacities tend to disappear as the ultrasound gain is decreased. However, the signals from asteroid bodies remain dispersed and highly reflective as the gain is lowered. Multiple, highly reflective spikes with independent movement are produced by the asteroid bodies during standardized A-scan evaluation. Ophthalmic ultrasound is also beneficial in monitoring patients diagnosed with infection and inflammation of the vitreous. If endophthalmitis is suspected, serial ultrasound examinations can be helpful in evaluating the density (increase/decrease) of the signals produced by the infectious process prior to and following treatment. Repeat echographic evaluation is also suggested to rule out the development of more sight-threatening complications such as retinal and/or choroidal detachments. In extreme cases of severe infection or inflammation, the entire globe and surrounding orbital tissue can be affected. The echographic findings of panophthalmitis include dense, dispersed vitreous opacities, marked thickening of the ocular coats and probable low reflective infiltration in or near the optic nerve, and Tenon’s capsule. Opacification of the vitreous gel can occur from several causes, such as aging, inflammation, infection, and hemorrhage from trauma or systemic disease. As the vitreous gel liquefies, contracture of the vitreous occurs and the posterior hyaloid face can separate from the retinal surface. Mobility of the vitreous gel can be easily evaluated with contact B-scan by having the patient move the eye. It is important to note that if the probe is being held in a vertical position, the patient should be instructed to move the eyes up and down. If the probe is oriented horizontally, the patient should be instructed to move the eyes left and right to keep the area of interest within the parameters of the sound beam. Generally, when there is partial or complete detachment of the posterior hyaloid surface from the retina, the posterior vitreous face will exhibit a distinct wavelike movement. It is important to systematically evaluate all areas of the globe as the patient moves the eye to identify focal areas of vitreoretinal adhesion (where the posterior hyaloid remains adherent to the retina). It is in these areas that retinal breaks or traction retinal detachments may occur. When the posterior vitreous face remains adherent to the optic disc, confusion between retinal detachment and vitreous membrane can occur. The posterior vitreous face does not always remain attached at the optic disc and has a weaker insertion in the periphery. Vitreous membranes display a smoother consistency than retina and appear more mobile on B-scan. Although retinal detachments and vitreous membranes can both appear dense on B-scan evaluation, vitreous membranes appear thinner on standardized A-scan and it may not be possible to maintain a maximally high signal. As a general rule, the retina remains attached at the optic disc and has very strong adherence to the fundus at the ora serrata. Usually retinal detachments have a more folded appearance on B-scan and almost always produce a 100% tall spike on standardized A-scan. This separate, highly reflective A-scan spike can be maintained from the posterior aspect of the fundus to the ora serrata. Following vitrectomy, some eyes may develop a vitreous hemorrhage. The echographer may notice even more mobility of the opacities within the vitreous cavity because the balanced salt solution present in a vitrectomized eye has a less thick consistency than vitreous gel. The vitreous skirt (residual peripheral vitreous face) may be noted in the periphery for 360 degrees but is more commonly noted inferiorly. It is not uncommon for vitreous hemorrhage to become layered (posterior hyphema) and mimic membrane formation, which can be confused with a localized area of retinal detachment. Generally, layered hemorrhage will move and change shape but retinal detachment will remain consistent in density and location. The movement of layered blood can be observed by having the patient move the eyes or by tilting the head while continuing to aim the sound beam in the direction of the area of interest. The echographer will observe the “puddle” of blood moving along the globe wall. If standardized A-scan is performed, a maximally high signal may be displayed; however, the spike will most likely be very thin, unlike a thicker spike produced by a retinal detachment. Fuller DG, Hutton WL. Pre-Surgical Evaluation of Eyes with Opaque Media. New York: Grune & Stratton; 1982 McLeod D, Restori M. Ultrasonic examination in severe diabetic eye disease. Br J Ophthalmol 1979;63(8):533–538 Ossoinig KC. Standardized echography: basic principles, clinical applications, and results. Int Ophthalmol Clin 1979;19(4):127–210 Ossoinig KC, Frazier SL, Watzke RC. Combined A-scan and B-scan echography as a diagnostic aid for vitreoretinal surgery. In: McPherson A, ed. Ew Controversial Aspects of Vitreoretinal Surgery. St. Louis: CV Mosby Company; 1977:106
The Vitreous
 Suggested Readings
Suggested Readings
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


