Country
Who, where
Particle
S/C/SCa Max. energy (MeV)
Beam directions
Start of treatment
Total patients treated
Date of total
Canada
TRIUMF, Vancouver
p
C 72
1 horiz.
1995
175
Dec-13
Czech Republic
PTC Czech r.s.o., Prague
p
C 230
3 gantries, 1 horiz.
2012
140
Dec-13
China
WPTC, Wanjie/Zibo
p
C 230
2 gantries, 1 horiz.
2004
1,078
Dec-13
China
IMP-CAS, Lanzhou
C-ion
S 400/u
1 horiz.
2006
213
Dec-13
England
Clatterbridge
p
C 62
1 horiz.
1989
2,446
Dec-13
France
CAL, Nice
p
C165
1 horiz.
1991
4,936
Dec-13
France
CPO, Orsay
p
S 250
1 gantry, 2 horiz.
1991
6,432
Dec-13
Germany
HZB, Berlin
p
C 250
1 horiz.
1998
2,312
Dec-13
Germany
RPTC, Munich
p
C 250
4 gantries, 1 horiz.
2009
1,811
Dec-13
Germany
HIT, Heidelberg
p
S 250
2 horiz., 1 gantryb
2009, 2012
503
Dec-13
Germany
HIT, Heidelberg
C-ion
S 430/u
2 horiz., 1 gantryb
2009, 2012
1,368
Dec-13
Germany
WPE, Essen
p
C 230
4 gantriesc, 1 horiz.
2013
32
Dec-13
Italy
INFN-LNS, Catania
p
C 60
1 horiz.
2002
350
Dec-13
Italy
CNAO, Pavia
p
S 250
3 horiz., 1 vertical
2011
76
Dec-13
Italy
CNAO, Pavia
C-ion
S 480/u
3 horiz., 1 vertical
2012
105
Dec-13
Japan
HIMAC, Chiba
C-ion
S 800/u
horiz.c, verticalc
1994
8,073
Dec-13
Japan
NCC, Kashiwa
p
C 235
2 gantriesc
1998
1,226
Mar-13
Japan
HIBMC, Hyogo
p
S 230
1 gantry
2001
4,223
Dec-13
Japan
HIBMC, Hyogo
C-ion
S 320/u
horiz.,vertical
2002
1,935
Dec-13
Japan
PMRC 2, Tsukuba
p
S 250
2 gantries
2001
2,967
Dec-13
Japan
Shizuoka Cancer Center
p
S 235
3 gantries, 1 horiz.
2003
1,590
Dec-13
Japan
STPTC, Koriyama-City
p
S 235
2 gantries, 1 horiz.
2008
2,306
Dec-13
Japan
GHMC, Gunma
C-ion
S 400/u
3 horiz., 1 vertical
2010
985
Dec-13
Japan
MPTRC, Ibusuki
p
S 250
3 gantries
2011
919
Dec-13
Japan
Fukui Prefectural Hospital PTC, Fukui City
p
S 235
2 gantries, 1 horiz.
2011
428
Dec-13
Japan
Nagoya PTC, Nagoya City, Aichi
p
S 250
2 gantries, 1 horiz.
2013
199
Dec-13
Japan
SAGA-HIMAT, Tosu
C-ion
S 400/u
3 horiz., vertical, 45 deg.
2013
62
Dec-13
Poland
IFJ PAN, Krakow
p
C 60
1 horiz.
2011
39
Dec-13
Russia
ITEP, Moscow
p
S 250
1 horiz.
1969
4,320
Dec-13
Russia
St. Petersburg
p
S 1000
1 horiz.
1975
1,386
Dec-12
Russia
JINR 2, Dubna
p
C 200d
1 horiz.
1999
995
Dec-13
South Africa
NRF—iThemba Labs
p
C 200
1 horiz.
1993
521
Dec-13
South Korea
NCC, IIsan
p
C 230
2 gantries, 1 horiz.
2007
1,158
Dec-13
Sweden
Uppsala
p
C 200
1 horiz.
1989
1,356
Dec-13
Switzerland
PSI, Villigen
p
C 250
2 gantriese, 1 horiz.
1984, 1996, 2013
7,045
Dec-13
USA, CA
Loma Linda
p
S 250
3 gantries, 1 horiz.
1990
17,829
Dec-13
USA, CA
UCSF
p
C 60
1 horiz.
1994
1,621
Dec-13
USA, MA
NPTC, MGH Boston
p
C 235
2 gantriesc, 1 horiz.
2001
7,345
Dec-13
USA, IN
IU Health PTC, Bloomington
p
C 200
2 gantriesc, 1 horiz.
2004
1,927
Dec-13
USA, TX
MD Anderson Cancer Center, Houston
p
S 250
3 gantriesc, 1 horiz.
2006
4,746
Dec-13
USA, FL
UFPTI, Jacksonville
p
C 230
3 gantries, 1 horiz.
2006
5,085
Dec-13
USA, OK
ProCure PTC, Oklahoma City
p
C 230
1 gantry, 1 horiz, 2 horiz/60 deg.
2009
1,364
Dec-13
USA, PA
UPenn, Philadelphia
p
C 230
4 gantries, 1 horiz.
2010
1,744
Dec-13
USA, IL
CDH Proton Center, Warrenville
p
C 230
1 gantry, 1 horiz, 2 horiz/60 deg.
2010
1,329
Dec-13
USA, VA
HUPTI, Hampton
p
C 230
4 gantries, 1 horiz.
2010
767
Dec-13
USA, NY
ProCure Proton Therapy Center, New Jersey
p
C 230
4 gantries
2012
512
Dec-13
USA, WA
SCCA ProCure Proton Therapy Center, Seattle
p
C 230
4 gantries
2013
86
Dec-13
USA, MO
S. Lee Kling PTC, Barnes Jewish Hospital, St. Louis
p
SC 250
1 gantry
2013
1
Dec-13
USA, CA
Scripps Proton Therapy Center, San Diego
p
C 250
3 gantries, 2 horiz.
2014
1
Feb-14
Nowadays, protons are an accepted treatment modality for tumors in difficult to treat locations, i.e., in the area of the skull base or along the spinal axis, also including sarcomas involving the thoracic chest wall, as well as malignancies in pediatric patients, where minimizing normal tissue radiation exposure is of paramount importance. Outcome analyses demonstrate very satisfying tumor control rates and at the same time low incidence of radiation-induced toxicities (Hug and Slater 2000; DeLaney et al. 2009; Rutz et al. 2008).
3 Physical Characteristics of Protons
PT with its physical characteristics of superior dose deposition in a given tumor and reduced radiation dose to surrounding normal tissues offers an inherent geometric advantage. Lower entrance doses as well as sharp dose falloff at the distal edge of the beam result in a significant higher conformality in comparison to photons. The main disadvantage of the proton beam is the worse lateral dose falloff and the range of uncertainties when treating tissues of different densities especially if there are inter- and intra-fractional changes during treatment (Fig. 1).
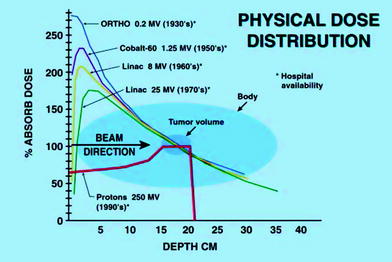
Fig. 1
Dose distribution of different beam qualities
4 Radio-Biological Effectiveness (RBE) of Protons
According to the International Commission on Radiation Units and Measurements (ICRU) report 78 (ICRU 2007) the radio-biological effectiveness (RBE) of protons is comparable with the RBE of photons. Dose units expressed as physical dose have a difference of about 10 % in favor of protons (Paganetti et al. 2002). The usually constant RBE of 1.1 in comparison to photons is an advantage of the proton beam. Nevertheless, one has to estimate a higher RBE at the distal edge of the proton beam. Also, the intensity of the linear energy transfer (LET) influences the RBE (see also the following chapter “There is Evidence of the Superiority of Protons or Heavy Ions, Pro”). Comparable proton or photon doses have a similar cell-killing effect on tumors and similar toxic effects on normal healthy tissues (Paganetti et al. 2004). This results in an excellent estimation of expected toxicities in comparison to applied doses during the treatment planning process. Established tolerance doses in RT are generally transferable to PT. All available publications on treatments with protons confirmed it. No publication has raised the issue of unexpected acute or late toxicity. Any described incidence of late toxicity was related to high dose escalation rather than use of protons. The initial concept of physical dose distribution and effectiveness has not been called into question by clinical results. However, no phase III trials were available comparing protons and photons. Most proton radiation therapy data were based on retrospective reviews and only for a few indications data were based on phase I/II trials of single institution experiences. Multi-institutional collaboration was very limited.
Related posts:
 Toxicity and Quality of Life
Treatment of the Pelvic Lymphatics in Patients with High-Risk Prostate Cancer: Pro Radiation
Radiotherapy After Radical Prostatectomy
is Evidence for the Superiority of Protons or Heavy Ions, Contra
Toxicity and Quality of Life
Treatment of the Pelvic Lymphatics in Patients with High-Risk Prostate Cancer: Pro Radiation
Radiotherapy After Radical Prostatectomy
is Evidence for the Superiority of Protons or Heavy Ions, Contra
 of Pelvic Irradiation
of Pelvic Irradiation
 Radiation Therapy for Clinically Localized Prostate Cancer
Radiation Therapy for Clinically Localized Prostate Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


