Congenital, developmental, and acquired conditions of the pediatric hip frequently present with sequelae in the adult. There is substantial overlap in the end-stage results of these pathologic conditions, including osseous changes, chondral/labral injuries, and premature osteoarthritis. This review discusses the top 10 etiopathogeneses of pediatric hip conditions and presents associated dysmorphisms in the adult on an illustrative, multimodality, case-based template. Quantitative imaging metrics and the role of advanced imaging techniques are reviewed. The ultimate goal is enhanced understanding of the expected evolution of childhood hip pathologic conditions and their associated complications for general radiologists.
Key points
- •
Pediatric hip pathologic conditions arise from various etiopathogeneses but frequently display common morphologic and functional outcomes.
- •
Specific radiographic views and quantitative imaging metrics are useful for assessing mechanics and congruity of the hip joint.
- •
Altered joint mechanics in the adult arising secondary to pediatric hip pathologic conditions can result in labral and chondral injury with premature osteoarthritis.
Introduction
To accurately assess the hip, the practicing radiologist should have familiarity with its anatomic components and the standard imaging techniques used to visualize them. The hip is a ball-in-socket joint with the femoral head articulating within the acetabulum. The femoral head and acetabulum are lined with hyaline cartilage to absorb shock and decrease friction during articulation. The fibrocartilaginous labrum attached to the bony acetabular rim both stabilizes the hip and seals in joint fluid to promote even load-bearing. Any incongruence in femoral head-acetabular articulation can promote uneven cartilage wear and weight-bearing and premature cartilage breakdown. Both femoral head dysplasia and acetabular dysplasia can result in pathologic weight-bearing, early breakdown of articular cartilage, labral loading and injury, proliferative bone formation leading to CAM (an abbreviation for “camshaft,” an automotive analogy describing the shape, which the femoral head and neck resembles) and pincer impingement, and premature osteoarthritis. These pathologic outcomes are common endpoints for a wide variety of different pediatric hip pathologic conditions.
This review discusses the top 10 etiopathogeneses of pediatric hip conditions and presents associated dysmorphisms in the adult on an illustrative, multimodality, case-based template. Quantitative imaging metrics and the role of advanced imaging techniques are reviewed. Imaging discussion is supplemented with case presentations, key radiology pearls, and discussion of treatment modalities. The ultimate goal is enhanced understanding of the expected evolution of childhood hip pathologic conditions and their associated complications for general radiologists.
Imaging techniques and normal anatomy
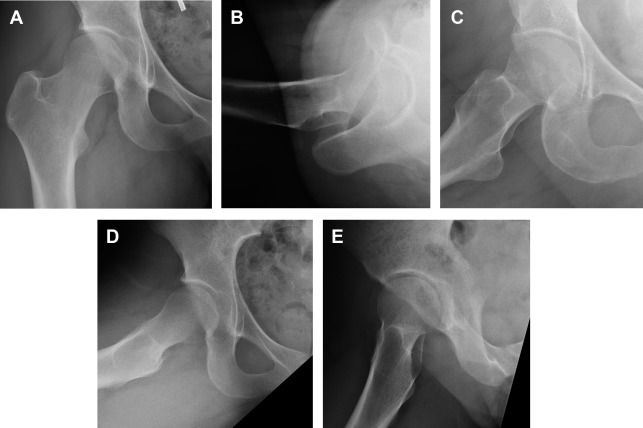
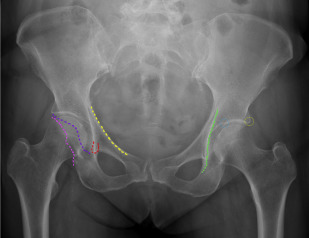
Five basic radiographic views are generally sufficient to accurately evaluate the adult hip: the anterioposterior (AP), lateral, frog-leg-lateral, Dunn, and false profile views ( Fig. 1 ). Radiographic technique for each of these views is summarized in Table 1 . Frequently referenced anatomic hip landmarks are summarized in Fig. 2 . Specific imaging metrics frequently used for quantitative analysis of plain radiographs of the hip are summarized in Table 2 . Excellent pictorial summaries of these metrics have been previously published. A summary of several of the more advanced imaging modalities commonly used to evaluate the adult hip is summarized in Table 3 .
| Projection | Patient Position | Tube Position | Clinical Utility | Quantitative Radiographic Metrics |
|---|---|---|---|---|
| AP | Supine Hips 15° internal rotation | Beam perpendicular to table at 120 cm Crosshairs centered between PS and ASIS | Acetabular morphology | Acetabular depth Acetabular version Acetabular index (sharp index) Tonnis angle LCEA (angle of Wiberg) Femoral head sphericity Femoral head lateralization Congruency |
| False profile | Standing Symptomatic hip against cassette Symptomatic foot parallel to cassette Pelvis 65° to cassette, facing beam | Beam perpendicular to patient at 102 cm Crosshairs centered on femoral head | Acetabular morphology | ACEA (angle of Lequesne) Congruency |
| Lateral | Supine Contralateral hip and knee flexed 80° Symptomatic hip 15° internal rotation | Beam parallel to table 45° to symptomatic limb Crosshairs centered on femoral head | Proximal femur | Femoral head sphericity Femoral head neck offset congruency |
| Frog-leg lateral | Supine Ipsilateral knee flexed 30°–40° Symptomatic hip abducted 45° Heel against contralateral knee | Beam perpendicular to table at 102 cm Crosshairs centered between PS and ASIS | Proximal femur | Femoral head sphericity Femoral head neck offset Alpha angle a Congruency |
| Dunn | Supine Symptomatic hip and knee flexed 90° Symptomatic hip abducted 20° | Beam perpendicular to table at 102 cm Crosshairs centered between PS and ASIS | Proximal femur | Femoral head sphericity Femoral head neck offset Congruency |
a Approximate; true angle traditionally measured on cross-sectional oblique CT or MR imaging.
| Imaging Modality | Normal | Clinical Significance (Abnormal) | Common Pertinent Hip Pathologic Conditions | |
|---|---|---|---|---|
| CAM deformity | ||||
| Alpha angle | Axial MR imaging or CT | <55⁰ | CAM deformity | LCPD SCFE Intraarticular osteoid osteoma of hip AIIS avulsion |
| Femoral head neck offset | Any lateral radiograph | >0.17 | CAM deformity | LCPD SCFE Intraarticular osteoid osteoma of hip AIIS avulsion |
| Pincer deformity, acetabular dysplasia | ||||
| LCEA | AP radiograph | 25°–40⁰ | Decreased: structural instability Increased: pincer impingement | DDH PFFD Charcot hip Inflammatory/infectious arthritis LCPD |
| ACEA | AP radiograph | 20°–45⁰ | Decreased: structural instability Increased: pincer impingement | DDH PFFD Charcot hip Inflammatory/infectious arthritis LCPD |
| Acetabular depth | AP radiograph | Floor of acetabulum does not abut/cross ilioischial line on AP radiograph | Pincer impingement | Infectious/inflammatory arthritis |
| Femoral head lateralization | AP radiograph | >10 mm | Structural instability | DDH Charcot hip |
| Acetabular index (Sharp index) | AP radiograph | <45⁰ | Structural instability | DDH PFFD Charcot hip LCPD |
| Tonnis angle | AP radiograph | 0°–10⁰ | Increased: structural instability Decreased: pincer impingement | DDH PFFD Charcot hip LCPD |
| Joint alignment | ||||
| Acetabular version | AP radiograph | 13°–20⁰ anteversion | Pincer impingement | SCFE |
| Femoral version | Axial MR imaging or CT | 8°–14⁰ anteversion | Excessive retroversion risk factor for poor outcomes after corrective FAI surgery | DDH FAI SCFE |
| Joint congruity | ||||
| Femoral head sphericity | AP and lateral radiograph | Any portion of femoral head >2 mm beyond standard Mose template | Joint wear and early OA | DDH PFFD Charcot hip LCPD Infectious/inflammatory arthritis IHC |
| Imaging Modality | Views/Sequences | Clinical Utility |
|---|---|---|
| Plain radiograph | AP Lateral Frog-leg lateral Dunn False profile | Evaluate acetabular and femoral morphology and congruence Preoperative and postoperative assessment Routine surveillance imaging |
| CT | Axial, coronal, and sagittal views 3D modeling | Assess complex fractures and hip dysmorphologies Preoperative planning with automated hip measurements Assessment of hip version |
| MR imaging | Conventional 3 T imaging: dedicated hip coils, parallel imaging, isotropic MR MR arthrography, ± traction Biochemical MR imaging: dGEMRIC, T2 and T2*, T1 rho, Na+ mapping 3D modeling Virtual ROM analysis Open MR imaging (functional imaging) 3D printing Advanced metal suppression MR fingerprinting | Assessment of cartilage and labral injuries Biochemical cartilage mapping (dGEMRIC, T2/T2*, T1 rho, Na + mapping) Automated analysis of joint parameters, for example, alpha angle via 3D modeling Subject-tailored preoperative virtual planning Dynamic ROM simulation Real time in vivo functional imaging |
Two scenarios are generally encountered when evaluating adult hip disease arising secondary to childhood hip pathologic conditions in daily clinical practice:
The disease process and pathophysiology are known, in which case the radiologist is following hip morphology for interval change.
The disease process is unknown, and the radiologist is evaluating hip morphology to assist in diagnosis of the underlying pathologic condition.
It is most helpful, therefore, to organize commonly encountered hip pathologic conditions by both morphology ( see Table 2 ) and etiopathogenesis ( Tables 4 and 5 ).
| Etiopathogenesis | Pathophysiology/Mechanism | Imaging Features | Abnormal Imaging Metrics | Possible Operative Findings |
|---|---|---|---|---|
| Developmental/congenital | ||||
| DDH | Lateralized femoral head Acetabular undercoverage | Coxa valga Femoral lateralization Hip subluxation AD Premature OA/cartilage damage | LCEA/ACEA Acetabular index Tonnis angle | Periacetabular osteotomy Femoral varus osteotomy Hip resurfacing arthroplasty Total hip arthroplasty |
| PFFD |
| Coxa vara Femoral head deformity Proximal femoral deficiency AD | LCEA/ACEA Acetabular index Tonnis angle | Various femoral lengthening procedures |
| Charcot hip a | Sensory/autonomic neuropathy Insensate bone imperceptible trauma Hyperemia bone breakdown | Femoral head deformity Femoral lateralization Pseudoarticulation AD Premature OA/cartilage damage | Acetabular index Acetabular depth Tonnis angle | Total hip arthroplasty |
a Congenital neuropathic hip most frequently related to spina bifida, Chiari malformations, and syringomyelia.
| Etiopathogenesis | Pathophysiology/Mechanism | Imaging Sequela | Abnormal Imaging Metrics | Possible Operative Findings |
|---|---|---|---|---|
| Acquired | ||||
| LCPD | Loss of blood flow to femoral head AVN Relative CAM deformity | Femoral head deformity CAM deformity AD Premature OA/cartilage damage | LCEA Acetabular index Femoral head neck offset ratio Alpha angle | Femoral varus osteotomy Periacetabular osteotomy Femoral neck lengthening Innominate osteotomy Shelf procedure |
| SCFE | Femoral head deformity CAM deformity Premature OA/cartilage damage | Acetabular version Femoral head neck offset ratio Alpha angle | Femoral head pinning Proximal femoral osteotomy Femoral head/neck osteochondroplasty | |
| Infectious/inflammatory arthritis |
| Femoral head deformity Femoral lateralization Coxa vara/valga Leg length discrepancy AD Joint ankylosis/heterotopic bone Premature OA/cartilage damage | Femoral head sphericity Tonnis angle Acetabular index Femoral head extrusion index | Pelvic acetabuloplasty Femoral varus/valgus osteotomy Epiphysiodesis with contralateral leg lengthening Trochanteric arthroplasty Total hip arthroplasty |
| IHC | Idiopathic rapid destruction of hip cartilage | Symmetric joint space narrowing Periarticular osteopenia Acetabular protrusion Joint ankylosis/heterotopic bone Premature OA/cartilage damage | Acetabular depth Acetabular index Tonnis angle | Total hip arthroplasty |
| Osteoid osteoma of the hip |
| Lucent nidus with surrounding sclerosis (minority of intraarticular cases) Coxa valga Widening of femoral neck (CAM deformity) Premature OA/cartilage damage | Alpha angle Femoral head neck offset ratio | Osteochondroplasty |
| Traumatic avulsion | Repetitive stress (athletics) Direct trauma | AIIS hypertrophy, malunion, or nonunion Heterotopic bone formation CAM deformity | Alpha angle (concurrent CAM deformity) Femoral head neck offset ratio | AIIS osteochondroplasty Femoral head/neck osteochondroplasty |
Related posts:
 Brain Malformations at All Ages
Brain Malformations at All Ages
 Repaired Congenital Heart Disease in Older Children and Adults
Repaired Congenital Heart Disease in Older Children and Adults
 Interstitial Lung Diseases in Children, Adolescents, and Young Adults
Interstitial Lung Diseases in Children, Adolescents, and Young Adults
 Cystic Fibrosis from Childhood to Adulthood
Cystic Fibrosis from Childhood to Adulthood
 Spectrum of Imaging Manifestations of Vascular Malformations and Tumors Beyond Childhood
Spectrum of Imaging Manifestations of Vascular Malformations and Tumors Beyond Childhood
 Congenital Incidental Findings in Children that Can Be Mistaken as True Pathologies in Adults
Congenital Incidental Findings in Children that Can Be Mistaken as True Pathologies in Adults
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


