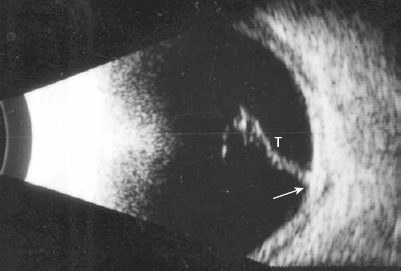
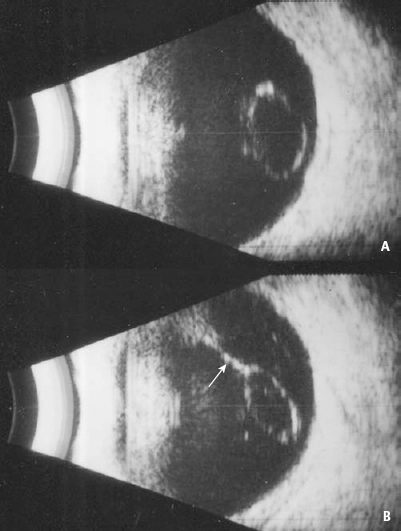
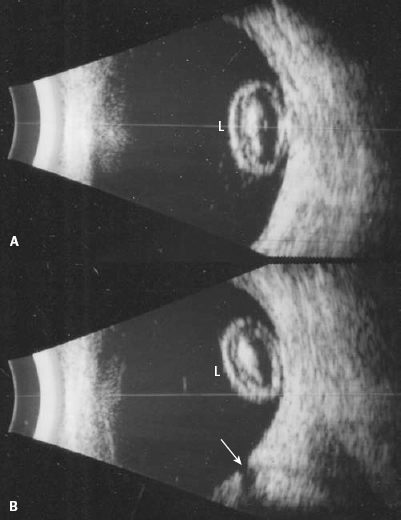
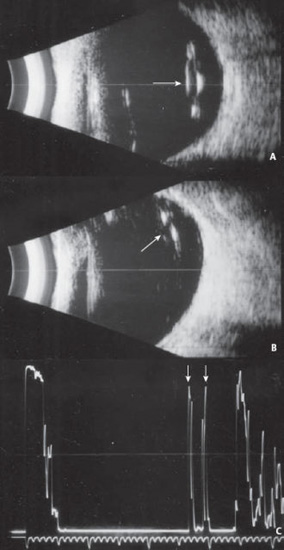
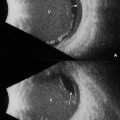
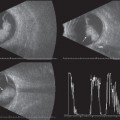
6 Echography can be a great aid to the ophthalmologist in the evaluation of the traumatized eye. Following ocular trauma, indirect ophthalmoscopy is frequently impossible because of the opacified media due to hyphema, cataract formation, vitreous hemorrhage, or edematous eyelids, and often poor patient cooperation. Echography can supplement the clinical findings by permitting evaluation of the intraocular structures that in turn may facilitate management and treatment. An attempt at complete ophthalmoscopic evaluation is necessary prior to echographic evaluation to determine whether the globe wall has been compromised. Surgical repair of the rupture site is generally performed before ultrasound is attempted. However, in some instances when an intraocular foreign body is suspected and the exact location cannot be confirmed with either plane films or computed tomography (CT) scan, a very gentle ultrasound examination through the lids may yield the necessary information to assist in the removal of the foreign body. This can be done in the operating room under sterile conditions if necessary. When an ultrasound examination is performed through the lids, a generous amount of methylcellulose is needed as a coupling agent so the echographer can apply a minimal amount of pressure on the globe while still obtaining useful information. Increasing the system sensitivity (gain) counterbalances the sound attenuation that occurs from the eyelids. As swelling and vitreous hemorrhage resorb, serial ultrasound studies may be necessary to confirm the initial findings. Green RL, Byrne SF. Diagnostic ophthalmic ultrasound. In: Ryan SJ, ed. Retina. Vol. 1. St. Louis: CV Mosby Company; 1989 Rubsamen PE, Cousins SW, Winward KE, Byrne SF. Diagnostic ultrasound and pars plana vitrectomy in penetrating ocular trauma. Ophthalmology 1994;101:809–814 Figure 6–1 Vitreous track. A small metal wire entered this eye, went through the vitreous cavity, and struck the posterior globe wall before the patient pulled it out. In this longitudinal scan, the track has hemorrhage lined up along it (T). There is a focal area of fundus thickening at the posterior impact site (arrow). (From DiBernardo C. Ultrasonography. In: Regillo CD, Brown GC, Flynn HW. Vitreoretinal Disease: The Essentials. New York: Thieme Medical Publishers; 1999. Reprinted by permission.) Figure 6–2 Dislocated lens. (A) Transverse scan shows the round, echolucent lens in the vitreous cavity. (B) Longitudinal view showing the dislocated lens being suspended by a hemorrhagic membrane (arrow). Figure 6–3 Dislocated lens. Patient with a blind, painful eye, sustained a blunt trauma and presented to the emergency room with an anterior chamber hyphema (A). Echographically, the lens (L) was cataractous and dislocated, (B). A total optic disc cup was also noted (arrow). Figure 6–4 Dislocated lens. This patient had a history of cataract surgery with an intraocular lens implant (IOL) prior to sustaining a blunt trauma from a fall. (A) Transverse scan showing the IOL in the vitreous cavity and an area of shadowing from the implant (arrow). (B)
Trauma
 Suggested Readings
Suggested Readings
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


