Gradea
Injury type
Description of injury
I
Hematoma
Subcapsular, <10 % surface area
Laceration
Capsular tear, <1 cm parenchymal depth
II
Hematoma
Subcapsular, 10–50 % surface area
Intraparenchymal, <5 cm in diameter
Laceration
Capsular tear, 1–3 cm parenchymal depth that does not involve a trabecular vessel
III
Hematoma
Subcapsular, >50 % surface area or expanding
Ruptured subcapsular or parenchymal hematoma
Intraparenchymal hematoma ≥ 5 cm or expanding
Laceration
>3 cm parenchymal depth or involving trabecular vessels
IV
Laceration
Laceration involving segmental or hilar vessels producing
major devascularization (>25 % of spleen)
V
Laceration
Completely shattered spleen
Vascular
Hilar vascular injury with devascularized spleen
26.2 Post-treatment Complication
26.2.1 Post-operative Complication
It has been reported that up to 40 % of all splenectomies are performed for iatrogenic injury. Excessive traction, injudicious use of retractors, and direct trauma during operations are typical mechanisms of injury. Splenic injury may occur in left hemicolectomy, open anti-reflux procedures, left nephrectomy, gastrectomy, and during exposure and reconstruction of the proximal abdominal aorta and its branches. The risk of injury to the spleen is higher in patients who have previously undergone abdominal surgery, in the elderly, and in obese patients.
26.2.2 Post-procedural Complication
Splenic injury is a rare complication of colonoscopy. However, given the increasing use of colonoscopy, it is worthy to be aware of this rare but potentially fatal complication of colonoscopy.
Splenic injury might also inadvertently occur during percutaneous nephrolithotomy. Ultrasound guidance during the procedure significantly reduces the risk of splenic injury. Cross-sectional imaging might be helpful in planning subcostal puncture by clarification of structures adjacent to the kidney. The possibility of splenic injury should be an immediate consideration in the event of hemodynamic instability after left-sided percutaneous nephrolithotomy.
26.3 Summary
1.
Splenic injury accounts for 25 % of all solid abdominal organ injuries.
2.
Computed tomography is the gold standard for the diagnosis of splenic trauma.
3.
The major role of ultrasonography in splenic trauma is for the postoperative patient and for long-term follow-up of patients treated conservatively.
4.
Splenic injury may occur in a variety of operative procedures.
5.
Splenic injury is a rare complication of colonoscopy and percutaneous nephrolithotomy.
26.4 Illustrations: Trauma and Post-treatment Complications of the Spleen
26.4.1 Splenic Contusion

Fig. 26.1
Splenic contusion in a 48-year-old male. Contrast-enhanced transverse CT shows a focal low-attenuating lesion (arrow) in the spleen. The lesion has disappeared on follow-up CT
26.4.2 Subcapsular Hematoma

Fig. 26.2
Subcapsular hematoma in a 33-year-old male. Contrast-enhanced transverse CT shows a crescentic hypoattenuating lesion (arrows) at the medial surface of the spleen
26.4.3 Splenic Laceration
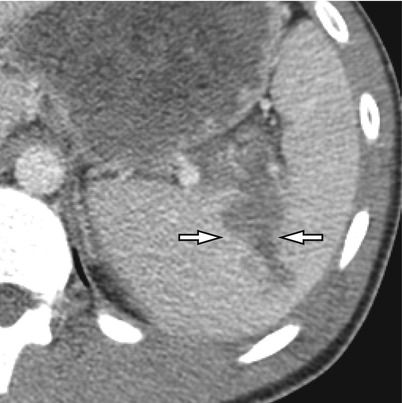
Fig. 26.3




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
