Trimalleolar Ankle Fracture
Andy K. Chon
Daniel B. Nissman
CLINICAL HISTORY
21-year-old man who fell on the ice after jumping off a ledge.
 FIGURE 28A |
 FIGURE 28B |
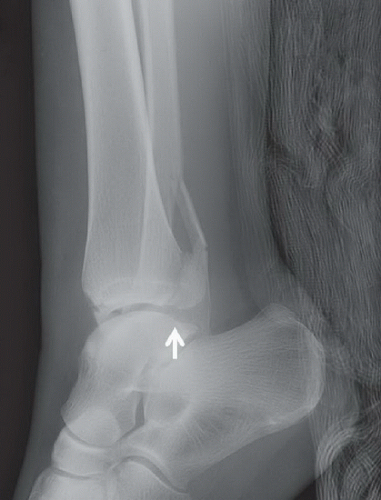 FIGURE 28C |
FINDINGS
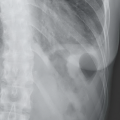
Supine anteroposterior (AP) radiograph of the ankle (Fig. 28A) demonstrates a transverse fracture through the medial malleolus (short arrow), and a fracture of the distal fibula above the level of the syndesmosis (long arrow). There is surrounding soft tissue swelling, greatest laterally. The ankle mortise view (Fig. 28B) reveals that the fracture of the distal fibula obliquely extends into the ankle mortise (arrow). The ankle mortise remains grossly approximated. The cross-table lateral view of the ankle (Fig. 28C) reveals a nondisplaced fracture of the posterior malleolus (arrow). Also demonstrated on the lateral view is mild posterior displacement and overriding of the oblique lateral malleolus fracture (arrow).
DIFFERENTIAL DIAGNOSIS
Inversion ankle injury, eversion ankle injury.
DIAGNOSIS
Trimalleolar ankle fracture secondary to eversion injury.
DISCUSSION
Ankle fractures are, along with hip fractures, one of the most common fractures of the lower extremity. One study from the United Kingdom found them to be ˜22% of all lower extremity fractures.1 Although most mechanisms result only in soft tissue injury, a percentage may also result in fractures that require more aggressive therapy. Published guidelines are available to help the clinician discern whether radiologic evaluation is warranted. These “Ottawa ankle rules” have been shown to demonstrate nearly 100% sensitivity in detecting fractures.2 According to these guidelines, imaging should be pursued only if there is tenderness over the malleolar areas or if there is pain significant enough to restrict weight bearing immediately after injury and also at the time of evaluation.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


