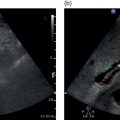
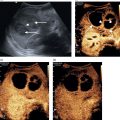
Matteo Rosselli1,2, Maija Radzina3,4,5, and Adrian K.P. Lim6,7 1 Department of Internal Medicine, San Giuseppe Hospital, USL Toscana Centro, Empoli, Italy 2 Division of Medicine, Institute for Liver and Digestive Health, University College London, Royal Free Hospital, London, UK 3 Radiology Research laboratory, Riga Stradins University, Riga, Latvia 4 Diagnostic Radiology Institute, Paula Stradins University Hospital, Riga, Latvia 5 Medical Faculty, University of Latvia, Riga, Latvia 6 Department of Imaging, Imperial College Healthcare NHS Trust, London, UK 7 Department of Metabolism, Digestion and Reproduction, Imperial College London, UK Biliary disorders include a variety of congenital and acquired pathological conditions that might be asymptomatic or present clinically with jaundice, abdominal pain, and fever in the case of biliary obstruction and superimposed infection. Ultrasound is the imaging modality of choice for a first differential diagnosis of jaundice in order to determine the presence, level, and cause of biliary obstruction. This chapter provides a brief introduction to the normal anatomy and topography of the biliary system, describing congenital abnormalities and anatomical variants, with a subsequent focus on benign and malignant pathologies. The gallbladder (GB) is a pear‐shaped structure, composed of a fundus, body, infundibulum, and neck (Figure 6.1). It is usually located on the visceral surface of the liver, along the major interlobar fissure between the right hepatic lobe and the medial part of the left one. In normal fasting conditions it is usually distended, thin walled (≤3 mm), and the lumen can clearly be visualised since it is filled with anechoic bile. When scanning the GB it is very important to keep in mind that its development might be affected by anatomical variants, resulting in a different size, number, shape, or location. Some malformations can lead to misdiagnosis and it is important to be aware of their presence in order to avoid incorrect clinical judgement and management. GB agenesis and hypoplasia [1] are rare congenital findings due to failure or incomplete development during morphogenesis. Agenesis is the complete absence of the GB, which is sometimes associated with other gastrointestinal and cardiovascular malformations and can manifest with right upper quadrant pain, often misinterpreted/misdiagnosed as biliary cholic secondary to cholelithiasis [2]. Hypoplasia is an incomplete development of the GB bud. When present it is often associated with other pathological conditions such as cystic fibrosis and biliary atresia [3]. Ectopic GB is a variation of its normal anatomical location. The most frequent positions are under the left lobe, intrahepatic, transverse, and retrohepatic [4]. It is important to bear in mind the possibility of an ectopic GB, since its unusual position can be mistaken for agenesis. In addition inflammation/infection of an ectopic GB can mimic different conditions. If surgery is indicated, this information is important because different GB locations may require different technical approaches. Phrygian cap GB is the most common anatomical variant, characterised by folding of the fundus on the body (Figure 6.2). The GB might present with septations, which can be partial or complete (Figure 6.3), leading to bile stasis, sludge, and stone formation (Figure 6.4). Multiseptate GB is a rare condition that leads to a multiloculated or honeycomb appearance [4]. Double or duplicated GB is also a rare congenital malformation. There are two main types of duplicated GB. The first corresponds to a bilobated GB with one common cystic duct that enters the common bile duct (CBD). The second is a true duplication that is also further classified into a first subtype in which two separate GBs have separate cystic ducts that independently enter the CBD; and a second subtype where two separate GBs have separate cystic ducts that join before entering the CBD. Ultrasound findings usually show two adjacent ‘cystic‐like’ structures within the GB fossa. However, ultrasound may not completely differentiate this from other conditions such as phrygian cap, choledochal cyst, folded GB, GB diverticulum, Ladd’s bands (intraperitoneal fibrous bands), and dilated cystic duct remnant. In addition, ultrasound may not be able to differentiate between the three variants and second‐level imaging such as magnetic resonance cholangiopancreatography (MRCP) is especially recommended if the patient needs to undergo cholecystectomy [5]. Figure 6.1 The gallbladder is composed of a fundus, body, infundibulum, and neck. Figure 6.2 Examples of a ‘phrygian cap’ of the gallbladder, which is characterised by folding of the fundus over the body. Figure 6.3 Septated gallbladder. The biliary tree is divided into intrahepatic and extrahepatic segments. The intrahepatic biliary tree is characterised by a canalicular network, interlobular ducts and main hepatic duct. The cystic duct originates as a direct continuation of the neck of the GB and joins the main hepatic duct to form the intrahepatic CBD. After a short tract, the CBD exits the liver (extrahepatic CBD), ending with the pancreatic duct in the ampulla of Vater at the level of the second part of the duodenum. The biliary ducts run across the liver together with the portal vein and hepatic artery from the periphery to the liver hilum, where they are enveloped in the hepatoduodenal ligament. The anatomical relationship of the hepatic artery and portal vein is important and must be kept in mind when considering and interpreting different causes of liver disease, as will be highlighted in the following sections. Figure 6.4 Septated thickened gallbladder containing sludge and stones (arrows). Cholelithiasis can be found on ultrasound as an incidental finding in asymptomatic patients or in those who typically present with right upper quadrant pain, associated or not with jaundice or fever in the case of biliary duct obstruction and infection. It is reported that the accuracy of ultrasound in diagnosing gallstones is almost 100%, with them appearing as highly reflective, well‐defined mobile structures of different shape and size that cast a posterior acoustic shadow (Figure 6.5) [6]. Nevertheless, it is important to bear in mind potential pitfalls, especially in symptomatic patients, since missed pathology and inappropriate management of cholelithiasis can lead to severe complications. False‐negative results more frequently occur when the stone size is very small (1–2 mm), when the stone calcium content is low or absent with significant reduction or no posterior acoustic shadowing (Figure 6.6), or in cases in which the stone is lodged in the neck of the GB or in the cystic duct. Changing the patient’s position can be very useful to improve visualisation of small or distal stones that might have been difficult to visualise because of overlying bowel gas. Alternatively, false‐positive results can be a consequence of side lobe and partial volume artefacts [7]. When a large stone or multiple stones completely fill the GB, the ultrasound image can be that of a wall‐echo‐shadow sign, characterised by a curvilinear or straight hyperechogenic line representing the GB wall, a thin hypoechoic space representing a small amount of bile, and a hyperechogenic line corresponding to the close surface of the gallstones with posterior acoustic shadowing [8]. The wall‐echo‐shadow sign needs to be differentiated from porcelain GB, in which complete or partial calcification of the wall occurs. In this case, the acoustic shadowing arises directly from the GB wall with no interposition (Figure 6.7). Figure 6.5 (a–c) Different examples of gallstones with typical posterior acoustic shadowing. In (b) a subtle layer of mobile sludge can be observed covering small stones accumulating in the infundibulum. Figure 6.6 (a) The gallbladder (GB) is filled with cholesterol stones with no acoustic shadowing. (b, c) A layer of small stones without acoustic shadowing accumulates along the posterior wall of the GB. Figure 6.7 (a) Porcelain gallbladder (GB). (b–d) Two examples of the wall‐echo‐shadow (WES) sign. In both cases, the GB is contracted and packed with stones. (d) reveals the appearance of the WES sign on a transverse scan view. Sludge refers to a bile precipitate with a sonographic appearance of echogenic homogeneous material without acoustic shadowing, which usually is mobile and accumulates in the most dependent portion of the GB following gravity. It can be a precursor of gallstones and it might present as isolated or mixed with gallstones (Figure 6.8). It can accumulate in the GB as a consequence of prolonged fasting and is often seen after prolonged total parenteral nutrition, or it might be associated with increased cholesterol levels, diabetes and haemolysis. Even in the absence of stones, biliary sludge can cause biliary obstruction, although the biliary system is usually not particularly dilated. Nevertheless, it can be responsible for cholecystitis, cholangitis, as well as pancreatitis. In the majority of cases biliary sludge is fluid and mobile and ultrasound can identify a clear interface between the sludge level and the ‘normal bile’. Alternatively it can completely fill the GB (Figure 6.8). Nevertheless, in other circumstances biliary sludge can solidify (Figure 6.8), appearing as a GB mass or pseudopolyp for which contrast‐enhanced ultrasound (CEUS) has high accuracy in differential diagnosis (Figure 6.9). Gallstones can impact the neck of the GB, causing obstruction and an inflammatory reaction with possible superimposed infection. The sonographic signs of lythiasic cholecystitis are GB wall thickening >3 mm, cholecystolithiasis, and a positive Murphy sign that refers to maximal tenderness, exacerbated by the pressure of the transducer over the GB (Figure 6.10) [6]. Hyperaemia on colour Doppler and pericholecystic fluid are reported as additional findings. Overdistension of the GB resulting in a longitudinal diameter >10 cm and a transverse diameter >4 cm can also be observed [6]. Nevertheless, increased GB size is not pathological per se and might be a physiological finding. In up to 15–20% of cases acute cholecystitis may be complicated by a gangrenous process, with a high probability of perforation and sepsis [9]. Ultrasound features are not specific but the clinical picture together with sonographic findings increases the diagnostic accuracy. In gangrenous cholecystitis, the GB wall has a striated and thickened appearance and intraluminal membranes can be observed as a consequence of wall detachment (Figure 6.11) [9, 10]. Moreover, marked asymmetry of the GB wall can often be seen, as well as echogenic debris within the GB lumen, together with pericholecystic collections (Figure 6.12). It is of note that frequently in the presence of gangrenous cholecystitis, Murphy’s sign can be negative, as a consequence of reduced GB intraluminal pressure. When perforation occurs, a defect in the GB wall is always present, although owing to the heterogeneous echogenicity of the inflammatory reaction and surrounding tissues, it can be difficult to delineate. An indirect sign can be the presence of loculated fluid collections surrounding the GB and liver. In cases of doubt, CEUS is extremely accurate in highlighting even small defects in the GB wall as a sign of perforation (Figures 6.13 and 6.14) (Videos 6.1 and 6.2). Figure 6.8 (a, b) The gallbladder (GB) is filled with sludge. (c) Sludge‐filled GB with large stones casting a typical acoustic shadow. (d) A clear interface is seen between sludge and anechoic bile. (e) Solidified sludge can be slightly mobile but is mostly adherent to the GB wall. Figure 6.9 The gallbladder (GB) lumen is filled with heterogeneous material that seems in direct continuity with the GB wall, suggesting a possible neoplastic growth (a). However, on contrast‐enhanced ultrasound the GB content does not show any enhancement thus excluding a neoplastic growth and steering the diagnosis towards solidified sludge (b). Figure 6.10 (a, b) A patient was admitted with right upper quadrant pain and fever. Ultrasound confirmed the diagnosis of acute gallstone cholecystitis based on the presenting symptoms and sonographic findings of gallbladder (GB) wall thickening and evidence of solidified sludge and stones accumulating in the GB neck, causing its obstruction. Both longitudinal and transverse planes show marked thickening of the GB wall compatible with the inflammatory process. Figure 6.11 (a–c) Ultrasound reveals detachment of the gallbladder walls, visualised as floating intraluminal ‘membranes’ and a discontinuity at the level of the fundus communicating with a collection (c, arrow), in keeping with gangrenous cholecystitis. Figure 6.12 (a) Acute cholecystitis in a septic patient presenting with right upper quadrant pain. Ultrasound highlights the intraluminal sludge, a thickened gallbladder (GB) wall, and a loculated pericholecystic collection (white arrows), orienting the diagnosis towards gangrenous cholecystitis with initial perforation. (b) The second sequence of images, taken after sudden hypotension and haemoglobin drop, revealed heterogeneous material almost filling completely the GB lumen, as well as thick, ill‐defined hyperechoic material surrounding the GB wall (black arrows). The features are in keeping with intraluminal and pericholecystic haemorrhage, likely caused by severe thrombocytopenia on a background of known myelodysplastic syndrome. Figure 6.13 (a–c) The gallbladder (GB) wall is thickened and the lumen is filled with heterogeneous material and a stone with clear posterior acoustic shadowing (white arrow). There is a pericholecystic collection adjacent to the left liver lobe (red arrow). However, while B‐mode ultrasound shows apparent integrity of the GB wall, contrast‐enhanced ultrasound (d–f) reveals a clear discontinuity, with leakage of the GB content in keeping with a perforated gangrenous cholecystitis (Video 6.1). Figure 6.14 Gangrenous cholecystitis. (a) The gallbladder (GB) lumen is replaced with heterogeneous material. There is loss of the normal GB wall that appears as a thin layer between the lumen and a circumferential collection. (b, c) Contrast‐enhanced ultrasound (CEUS) reveals that there is almost no enhancement of the GB wall, suggesting that it is likely necrotic. (d) CEUS helps to define the boundaries of the resulting collection that has a more loculated appearance at the level of the fundus (Video 6.2). Emphysematous cholecystitis is a severe complication of acute cholecystitis secondary to gas‐ forming bacteria. It may be associated with cholelithiasis, but also with acalculous cholecystitis and is more commonly associated with diabetes mellitus [9]. It is typically characterised by air in the GB lumen, wall or in an adjacent hepatic collection, in cases of perforation. Air in the GB can be seen on ultrasound as a curvilinear hyperechoic band with reverberation artefacts that accumulate anteriorly just below the GB wall (Figure 6.15) (Video 6.3). If there has been a perforation, gas‐related artefacts can be identified within the wall. Alternatively, comet‐tail artefacts related to gas bubbles with the tendency to accumulate in the anterior space of the GB lumen can be seen scattered within echogenic suppurative material. Emphysematous cholecystitis can easily be complicated by perforation and has a higher mortality rate, hence its recognition and correct management are crucial [11]. A biloma is an intra‐ or extrahepatic bile collection secondary to a GB or biliary duct leak. Bilomas can be caused by perforation as a consequence of acute cholecystitis (Figure 6.16) or as a complication of severe abdominal trauma involving the liver and biliary structures. Alternatively, a biloma may be a consequence of biliary and GB damage secondary to interventional procedures such as liver biopsy, endoscopic retrograde cholangiopancreatography (ERCP), or surgical intervention [12, 13]. Figure 6.15 There is thickening of the gallbladder (GB) wall and evidence of reverberation artefacts rising from the GB wall and the fundus, in keeping with an emphysematous cholecystitis (Video 6.3). Figure 6.16 (a) Multiple small stones accumulate in the gallbladder (GB) neck. (b) There is evidence of a large heterogeneous hepatic collection with both anechoic and echogenic content and debris. (c) The collection is aligned and in direct continuity with the GB neck, revealing a similar content, hence suggesting the diagnosis of GB perforation and biloma.
6
Ultrasound of the Biliary System
Anatomy and Topography of the Gallbladder and Biliary Tree




Gallbladder Pathology
Cholelithiasis



Biliary Sludge
Cholecystitis
Gangrenous Cholecystitis










Emphysematous Cholecystitis

Biloma



Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


