Ultrasound is the best imaging modality for comprehensive evaluation of the thyroid. The thyroid is best imaged using a high-frequency linear probe with the patient in a supine position with the neck hyperextended. Normal thyroid is homogeneous in appearance without defining anatomic landmarks within the gland. A few anatomic variants can occur, and it is important for the sonographer and radiologist to be aware of these variants, to avoid misidentifying them as a pathology. This article provides a comprehensive review of ultrasound of the normal thyroid gland, including technique, normal anatomy, anatomic variants, imaging appearance, and technical pearls and pitfalls.
Key points
- •
Ultrasound is the best screening and diagnostic test for evaluation of the thyroid gland.
- •
Thyroid ultrasound is best performed with the patient in a supine position with the neck hyperextended.
- •
The normal thyroid gland is homogeneous in appearance.
- •
There are a few anatomic variants to consider when imaging the thyroid gland as to not mistake normal anatomy for pathology.
Introduction
The thyroid is a superficial structure in the anterior neck. Because of this superficial location, ultrasound is the imaging modality of choice for evaluation of the thyroid gland. It is safe, inexpensive, and an effective diagnostic test. Furthermore, the components of ultrasound of the thyroid gland are well established, including the appearance of the normal thyroid gland and thyroid pathology.
Imaging protocols
The thyroid is imaged using a high-frequency linear transducer (7–15 MHz) with the patient lying supine with the neck in hyperextension. Placing a rolled towel beneath the upper shoulders can help extend the neck in larger patients or in patients with a low-lying gland. Ideally, the highest frequency available should be used to evaluate the thyroid gland; however, in certain clinical circumstances the frequency should be decreased to optimize tissue penetration. Both lobes should be imaged in transverse and longitudinal planes, and the isthmus should be imaged in the transverse plane. Measurements should be obtained for each lobe including the anteroposterior, transverse, and sagittal dimensions. The anteroposterior dimension of the isthmus should be measured in the transverse plane. Color Doppler images are obtained to supplement gray scale images in the appropriate clinical setting (ie, suspected thyroiditis) and to help characterize a focal abnormality or nodule. Imaging should also extend superiorly in the midline to detect a pyramidal lobe or thyroglossal duct cyst.
A complete evaluation of the thyroid also includes imaging of the internal jugular lymph node chain bilaterally to assess for the presence of enlarged or abnormal-appearing lymph nodes. The bilateral internal jugular chains are imaged in the transverse plane from the clavicle to the level of the hyoid (levels III, IV, and VI). Any enlarged benign-appearing lymph nodes or abnormal-appearing lymph nodes of any size are measured in three planes (anteroposterior, transverse, sagittal). Because enlarged benign-appearing lymph nodes are commonly identified in levels IA and IB and are almost universally related to the mouth and not the thyroid, these levels are not included in the standard thyroid protocol.
Imaging findings
The thyroid is a bilobed structure in the neck that is located anterior to the trachea, with the lobes extending vertically along the right and left sides of the trachea ( Fig. 1 ). The isthmus is the portion of the thyroid gland that connects the two lobes anteriorly. The trachea lies immediately posterior to the isthmus and is air-filled. Posterolateral to the thyroid lobe on each side is the carotid sheath, containing the common carotid artery medially and internal jugular vein laterally. Immediately anterior (superficial) to the thyroid are the strap muscles. The strap muscles include the sternohyoid and sternothyroid anterior to the thyroid, the sternocleidomastoid muscles anterolateral to the thyroid, and the longus colli muscles posteriorly. The esophagus is most commonly located posterior to the left lobe of the thyroid and can contain air ( Fig. 2 ). When evaluating the thyroid in the context of pathology that the thyroid lacks a true capsule, it does typically have a well-defined peripheral margin.


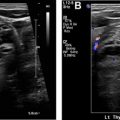
Sonographically, the normal thyroid gland is homogeneously echogenic with increased echogenicity as compared with the adjacent strap muscles. There are no specific anatomic landmarks within the thyroid. The size of the normal thyroid gland is variable, but in adults, each lobe measures approximately 5 × 2 × 2 cm (sagittal × anteroposterior × transverse) with the isthmus measuring up to 0.3 cm in anteroposterior dimension. A thyroid gland that is larger than these measurements is typically considered enlarged. An additional imaging finding that can further suggest that the thyroid is enlarged is bulging of the anterior surface of each lobe because this surface is typically symmetric and flat appearing ( Fig. 3 A). Extension of the gland over the anterior surface of the common carotid artery on a transverse image is evidence of gland enlargement ( Fig. 3 B). The normal thyroid gland can also extend over the surface of the carotid, but the anterior contour is typically flat. In children, gland shape and contour are used to indicate gland enlargement rather than size.

Sonographic evaluation of lymph nodes in the mid and low neck (levels III, IV, and VI) should be part of every thyroid ultrasound. Size and sonographic characteristics of the nodes should be assessed. Although size criteria are varied, at our institution a lymph node is considered enlarged if it measures greater than or equal to 7 mm in transverse diameter. Size and location of benign nodes meeting the criteria for enlargement are included in the report. Sonographic characteristics that are highly correlated with benign etiologies include an elongated shape, tapered or pointed ends, and a thin echogenic hilum. Color Doppler is used to visualize a single vessel entering the node at the hilum and branching toward each end of the node.
Anatomic variants
- •
Pyramidal lobe : Appears as normal thyroid tissue that arises from the isthmus and extends superiorly, anterior to the trachea. It may lay slightly to the right or left of true midline ( Fig. 4 ). It is important to recognize and report this normal variant, because nodules can occur in this lobe, and it could potentially be overlooked by the surgeon during a thyroidectomy.