MR imaging protocols and technical parameters should be optimized in order to achieve the best diagnostic results. Routine hip MR imaging includes a combination of T1-weighted and fluid-sensitive sequences, obtained in coronal, axial, and sagittal planes. MR arthrography of the hip can be used for assessment of intra-articular pathology involving intricate and signal-poor structures such as articular cartilage, labral fibrocartilage, and intra-articular bodies. Emerging quantitative MR imaging techniques such as T1ρ, T2 mapping, and delayed gadolinium-enhanced MR imaging of cartilage allow for the assessment of biochemical changes associated with cartilage degeneration and osteoarthritis.
Key points
- •
Routine hip MR imaging protocols typically include a combination of T1-weighted and fluid-sensitive sequences, which can be obtained in axial, coronal, and sagittal planes.
- •
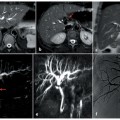
Radial images can improve assessment of complex 3-dimensional anatomy in the hip, offering improved visualization of the anterosuperior and posterosuperior labrum and improving detection of cam-type deformity.
- •
Direct MR arthrography can be useful for evaluation of intra-articular pathology, such as acetabular labral tears, chondral defects, and intra-articular bodies.
- •
Emerging quantitative MR imaging techniques such as T1rho, T2 mapping, and delayed gadolinium-enhanced MR imaging of cartilage allow for the assessment of biochemical changes associated with cartilage degeneration and osteoarthritis.
Introduction
MR imaging is an accurate and effective modality for the evaluation of a wide range of conditions affecting the hip. For disorders involving soft tissues such as the acetabular labrum, muscles, and tendons, MR imaging is often the preferred method of imaging given its high spatial resolution and image contrast, ability to image deep structures, and sensitivity for soft tissue edema and fluid. MR imaging can be used to diagnose and stage pathology ranging from occult fractures, osteonecrosis, bone and soft tissue tumors to rheumatological conditions, infections, degenerative arthropathy, sports injuries, and femoroacetabular impingement (FAI).
MR imaging protocols and parameters should be optimized, in order to achieve the best diagnostic results. Appropriate coil and field strength selection can be tailored to the patient and diagnostic question at hand to generate high-quality diagnostic images. Standard imaging sequences typically include a combination of T1-weighted and fluid-sensitive sequences, obtained in axial, coronal, and sagittal planes. Radial imaging and 3 dimensional (3D) volumetric sequences can assist in the evaluation of the complex 3D anatomy of the hip. For evaluation of intra-articular pathologies such as labral tears, chondral defects, and intra-articular bodies, MR arthrography may be appropriate and useful for improving diagnostic accuracy.
Emerging advanced techniques in hip MR imaging are enhancing the ability to assess early biochemical changes in cartilage associated with osteoarthritis, incorporating metabolic data, and improving image quality. Quantitative parameter mapping (QPM) techniques such as T1rho and T2 mapping have gained significant traction due to their relative simplicity and effectiveness in detecting biochemical alterations associated with osteoarthritis (OA). These technical advances continually increase the impact and effectiveness of hip MR imaging for the evaluation of a broad array of clinical problems.
Technical considerations
Field Strength
Diagnostic MR images of the hip can be obtained with low, medium, or high field strength systems. High field strength magnets (1.5 T and higher) are generally preferred because they have higher signal-to-noise ratios (SNRs) than lower field magnets, generating high-resolution images in shorter amounts of time. Lower field strength systems may be preferable in cases where patients have a metal prosthesis or other hardware, and in pregnant patients to reduce energy deposition.
Coil Selection
Initial screening with large field of view (FOV) images of the entire pelvis can be obtained with a phased-array body coil. High-resolution images of a single hip require the use of a local coil such as smaller field of view wrap coil, multiple channel cardiac coil, or commercially available or custom-built phased arrays. ,
Patient Positioning
Imaging is performed with the patient in supine position, with the imaged hip centered in the magnetic field. , The patient’s feet may be internally rotated and immobilized with tape, if necessary.
Routine imaging protocol
Standard Sequences
Initial large field-of-view short-tau inversion recovery (STIR) or T2-fat suppressed images of the entire pelvis, including the pubic symphysis, sacroiliac joints, lower lumbar spine, pelvic musculature, and viscera, can be useful to assess for extra-articular sources of hip and groin pain. , Large FOV images also allow assessment of contralateral hip disease and side-to-side comparisons of findings in the hips. Smaller FOV sequences of the symptomatic hip can then be obtained, with pulse sequences tailored to the clinical questions at hand. A typical imaging protocol of the pelvis and hips might include coronal spin-echo (SE) or fast SE (FSE) T1-weighted and fat-suppressed, FSE T2-weighted or STIR sequences, and transverse T1-weighted and T2-weighted sequences. T1-weighted images are useful for demonstrating anatomic detail and assessing fracture lines, marrow-replacing diseases, and muscle atrophy. Sagittal images are essential for evaluating anterosuperior labral tears and chondrolabral separation, and they can also be useful for quantifying the extent of femoral head osteonecrosis, evaluating hip joint cartilage, and assessing the proximal hamstring muscles and tendons.
Fluid-sensitive sequences are typically performed with an intermediate echo time (TE) that is high enough to make fluid and edema conspicuous, but low enough to visualize normal anatomy. Moderate TE with TEs between 30 and 40 milliseconds at 1.5 T and at 28 milliseconds at 3 T has been reported to provide excellent labral and cartilage contrast , ( Tables 1 and 2 ).
| Routine Hip w/o Contrast | |||||||
|---|---|---|---|---|---|---|---|
| Sequence | FOV (mm) | Slice Thickness (mm) | Gap (mm) | Matrix | Time (Estimate) | Notes | TI |
| Cor T1 TSE | 350 | 5 | 1 | 448 × 252 | 0:03:39 | Bilateral | |
| Cor STIR | 350 | 5 | 1 | 320 × 180 | 0:03:05 | Bilateral | 150 |
| Axial PD FS | 380 | 5 | 1 | 384 × 250 | 0:04:41 | Bilateral | |
| Axial T1 Oblique | 200 | 3 | .6 | 256 × 218 | 0:03:32 | Affected side | |
| Sag PD FS | 200 | 3.5 | .9 | 256 × 192 | 0:03:37 | Affected side | |
| Axial PD FS-Straight | 200 | 3 | .6 | 320 × 224 | 0:04:19 | Affected side | |
| CorPDFS | 180 | 3 | 1 | 256 × 256 | 0:04:19 | Affected side | |
| 3T Hip Arthrogram | |||||||
|---|---|---|---|---|---|---|---|
| Sequence | FOV (mm) | Slice Thickness (mm) | Gap (mm) | Matrix | Time (Estimate) | Notes | TI |
| 3 PLANE LOC | 400 | 5 | 256 × 192 | 0:00:23 | Bilateral Coverage | ||
| COR T1 WHOLE PELVIS | 360 | 5 | 1 | 384 × 224 | 0:03:31 | Bilateral Coverage | |
| COR STIR SPAIR | 360 | 5 | 1 | 384 × 224 | 0:03:51 | Bilateral Coverage | 30–40 |
| SAGT1 FS | 180 | 3 | 1 | 352 × 224 | 0:04:35 | Unilateral | |
| AX T2 FS straight | 180 | 3 | 1 | 352 × 224 | 0:04:22 | Unilateral | |
| COR T1 FS | 180 | 3 | 1 | 352 × 224 | 0:04:35 | Unilateral | |
| AX T1 FS STRAIGHT AX— For Patients at the Age of 50 and over | 180 | 3 | 1 | 352 × 256 | 0:04:23 | Unilateral | |
| AX OBLIQUE T1 FS— For Patients under 50 Years | 180 | 3 | 1 | 352 × 256 | 0:04:23 | Unilateral | |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


