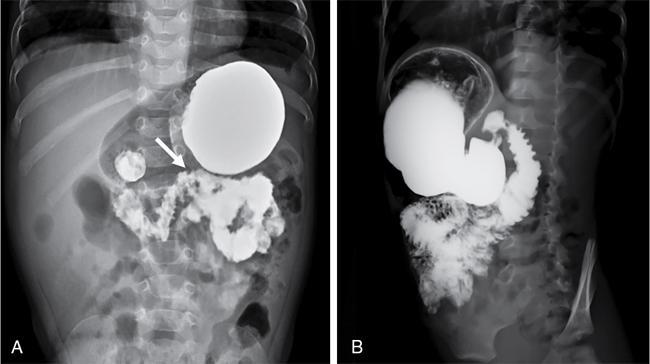
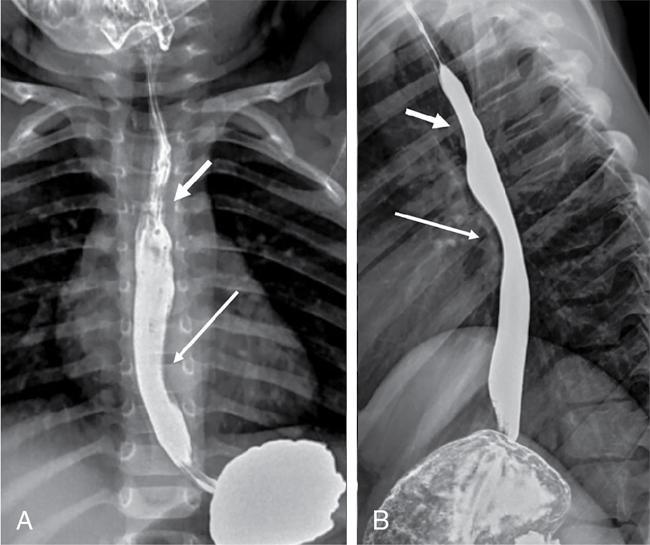
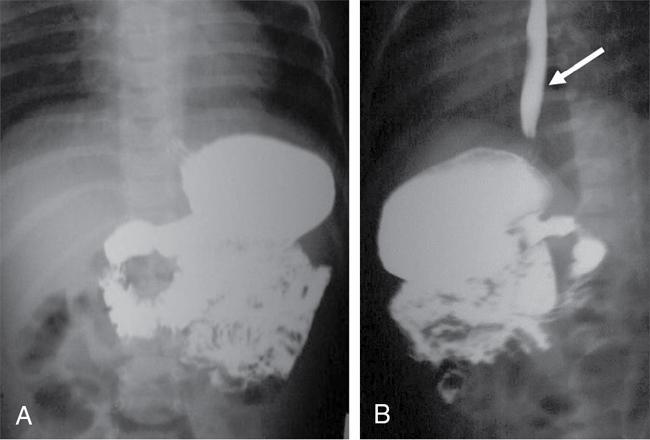
S. Muralinath, C.V. Kanimozhi, Krishnarjun M The focus and ambit of this chapter are restricted to the oesophagus as a subsequent author is dealing with the upper GI tract. Hence the narrative is confined to common problems like GER/GERD, achalasia, hiatus hernia, corrosive injury and ingested foreign bodies seen typically in infants and young children. The oesophagus is actually an anatomic and functioned continuum that serves essentially as a conduit between the hypopharynx and stomach. One cannot study the oesophagus in isolation without basic knowledge of the preceding structures and the following organs. Hence a brief consideration of the same is done along with the study of the oesophagus. The oesophagus basically transports the oropharyngeal contents onto the stomach. It goes without saying that there is bound to be an overlap or spillover of the proximal oropharyngeal and distal gastric disease onto the oesophagus. Dysphagia could be oropharyngeal or oesophageal and vomiting or regurgitation could be oesophageal or gastric. Hence the discussion will consider relevant proximal and distal elements in brief. Radiology and imaging play a significant role in the evaluation of children with upper GI tract diseases and is one of the most important sources of information for the clinician in the evaluation of GI tract diseases. The history and physical examination are crucial, but imaging plays a vital role in the assessment of GI tract disease. A plethora of investigative modalities are at one’s disposal today; hence, a good rapport between the clinician and the radiologist is essential in choosing the right investigations. Despite the advances in imaging technology and sophistry in techniques, the vast majority of the upper GI tract diseases in children, thankfully require only a few basic studies – conventional radiology (plain X-rays, fluoroscopy and contrast studies) and ultrasound. The downside is that in paediatric practice, these studies require in abundance practice and skill. Radiographic and fluoroscopic examinations are the mainstay in the study of upper GI tract disease in children. A preliminary plain film is the usual starting point; this supplemented by a few simple contrast studies and ultrasonography is all that is needed in the evaluation of most of the common upper GI tract diseases in children. It is mandatory that upper GI tract studies be done under fluoroscopic monitoring, as vital information is gained through the dynamics observed and the study is actively monitored and tailored to suit the clinical need. Barium is still the most commonly used contrast medium. Water-soluble contrast media are considered in specific circumstances as they are of value when the possibility of extravasation or perforation exists – for example, post-op evaluation of TEF repair. In the study of the oesophagus, hyperosmolar (ionic) contrast media are seldom utilized, as they may cause pulmonary oedema in the event of an aspiration. Nonionic low osmolar contrast media are preferred; especially in the newborn and young infant, because of the impact of ionic hyperosmolar contrast media on the water electrolyte equilibrium. To recognize the abnormal one has to realize the normal. The oesophagus is a relatively straight, hollow tube that follows the contour of the spine from the hypopharynx in the neck to the stomach in the abdomen. It has a relatively short cervical and abdominal segment with a long intervening thoracic component. It is governed at either end by high pressure zones. The upper oesophageal sphincter (UES) is defined by the cricopharyngeus, whereas the lower oesophageal sphincter (LES) is a poorly defined anatomic zone that is at and above the oesophago-gastric junction, partly straddling the diaphragmatic hiatus. The oesophagus has an inner mucosal layer lined mainly with stratified squamous epithelium which has negligible secretory and absorptive function. The outer muscular component has an external layer of longitudinal fibres and an internal layer of circular fibres. The musculature of the upper third is striated, whereas, in the lower third, it is nonstriated smooth muscle. The intervening segment is one of transition from the striated to the nonstriated. This nature of muscle distribution accounts for the central nervous system disorders affecting the motility of the pharynx and upper oesophagus, whereas autonomic system dysfunction leads to affliction of the lower oesophagus and the oesophago-gastric junction. The oesophagus at rest is in a collapsed state, bound at either ends by the UES and LES, respectively. These physiologic sphincter mechanisms maintain a tonic squeeze at rest generating a high pressure zone that prevents retrograde flow of contents from the oesophagus or the stomach. The function of the oesophagus is to propel contents from the pharynx onto the stomach. This is achieved through the mechanism of peristalsis. The pacemaker for the aboral, primary peristalsis is the act of deglutition. This once initiated travels down to the stomach. Peristalsis consists of a circular constrictive wave preceded by a wave of relaxation. This complex motor sequence is the result of the exquisite and intricate neural circuit (Auerbachian and Meissner plexuses) performing flawlessly in the gut wall. This wave drives the content in an aboral direction. While primary peristalsis is initiated by the act of swallowing, secondary peristalsis occurs in response to local oesophageal stimulus, the primary one being distention. This compliments the primary peristalsis in clearing the content. These propulsive mechanisms make sure that nothing stays in the oesophageal lumen, thus preventing stasis and its attendant complications. At rest, oesophagus is always kept in a collapsed state with no contents. Diagnostic tests commonly used in the evaluation of the oesophagus are oesophagogram, endoscopy and manometry. Endoscopy is for evaluating the oesophageal morphology, especially that of the lumen and the mucosa. Manometry offers information regarding the motor function; whereas an oesophagography provides information regarding both morphology and motor function and is usually the initial study in the evaluation of oesophagus. Barium is still the preferred contrast medium as it has the ability to provide a superior mucosal coating than any other contrast media. This coupled with its inherent density offers excellent contrast and detail. Barium is an inert substance with no adverse effect in the GI tract but that is not so when it leaks out and barium peritonitis is a much dreaded event. Water soluble low osmolar nonionic contrast media are considered when barium is contraindicated as in perforation. Water soluble hyperosmolar ionic contrast media are seldom used in paediatric practice as they cause airway and pulmonary compromise in the event of an aspiration. In newborn and young infants it can have a significant adverse effect on the water electrolyte equilibrium. The sole exception could be as therapeutic enema in meconium related disorders. Generally in paediatric practice a contrast swallow is seldom done in isolation. It is always a component of the upper GI series. The study is mostly done to evaluate vomiting or dysphagia. The problem could be in the oesophagus or elsewhere, for dysphagia could be pre-oesophageal and vomiting could be post-oesophageal. Contrast swallow may be done in isolation on follow-up studies, such as in post corrosive stricture, when the pathology has been localized, to evaluate the outcome of management. Be it a contrast swallow or an upper GI study, fluoroscopy is mandatory. Basic fluoroscopy and radiographic examination is the bedrock, when it comes to imaging evaluation of the oesophagus. An oesophagogram, as is the norm is done in conjunction with the upper GI series; wherein the mechanism of swallowing, the dynamics of peristaltic transit of content through oesophagus, stomach, duodenum and the proximal small bowel is studied along with it is morphology. Evaluation of the duodenum and DJ flexure is crucial for the documentation or exclusion of the rotational anomalies of the gut (Fig. 7.9.1). A standard operating protocol in a paediatric radiography suite would be: In children, especially the young ones, the oesophagus is a relatively simple structure and the mucosal folds are not that evident as in adults during a contrast swallow. But one can see often the extraneous impression caused by the aortic arch, the left main bronchus and the normal left atrium (Fig. 7.9.2). Normal peristalsis can be observed with the constricting ring preceded by the wave of relaxation leading to the aboral transmission of contrast. The peristalsis though, may not be as vigorous as in grownups. A word of caution during fluoroscopy – in the newborn and young infants the mediastinum and its structures are quite flexible and the oesophagus rather pliant. This will result in a peculiar configuration of the oesophagus during respiration. This is especially so if the infant cries leading to a bizarre and tortuous appearance of the oesophagus. To begin with this may be startling, but the entire process will settle once the crying induced Valsalva and the resultant elevation of intra-thoracic pressure eases. For the uninitiated a static film taken without fluoroscopy will be bewildering when viewed. Remember fluoroscopy is a must in paediatric upper GI study. A point to note is, small amounts of air in the oesophagus is not an uncommon finding in infants as they are quite aerophagic while feeding or even otherwise. Gastrooesophageal reflux (GER), hiatus hernia and achalasia cardia are considered in continuum as they essentially represent altered states at the same anatomic site – the oesophago-gastric junction. The literature on the anatomy and the physiology of the oesophagogastric junction is quite exhaustive; despite the various and numerous studies, the normal function of this junction defies clarity. GER as the name implies is the passage of gastric contents across the gastro-oesophageal junction into the oesophagus. The precise mechanism by which, aboral, unidirectional transit of content occurs at the oesophago-gastric junction is still not clearly understood. Various factors and mechanism are said to play a part in the valve like function of the oesophago-gastric junction. Apparently, the most important factor is the high pressure zone in the lower oesophagus representing the LES. A segmental tonic mechanism is considered to be operative in maintaining the high pressure. The other contributory factors said to assist mechanically are, the pinch-cock effect of the decussating crural fibres of the diaphragm, the unique anatomy of the junction providing the angle of His, the mucosal flap-valve mechanism, the posterolateral location of the fundus and the length of the intra-abdominal oesophagus. Transient relaxation of the LES is considered to be the primary mechanism by which reflux is said to occur. An autonomic, vagus mediated reflex regulates the transient relaxation of the LES. This relaxation reflex can be initiated by gastric-distention or by the initiation of swallow even when not leading to oesophageal peristalsis. The diagnosis of GER is made on a clinical basis from the history and physical examination. GER in a healthy, thriving infant is a physiologic and self-limiting entity. It is mostly managed by empirical and conservative measures along with parental reassurance. It is essential to differentiate physiologic GER from the pathologic state – GER disease (GERD). In GERD, as the name implies, the infant or child is no longer at ease. When GER is frequent and persistent leading to troublesome symptoms or complications, then what you have at hand is GERD. GER can have GI symptoms as well as non-GI related symptoms, like the oft stated peculiar manifestation of neck contortions in Sandifer’s syndrome. Reflux of acid content on to the airway may cause apnoea, cyanotic spells and the much dreaded sudden infant death syndrome. Another subset is there with silent or occult GER. In these infants or children, the GER does not manifest as regurgitation, vomiting or rumination. It is because these reflux does not quite reach the oral cavity to manifest as symptoms and yet could potentially be as harmful. Hence investigation is done to evaluate occult GERD and in high risk groups (neurological disorders, trisomy 21 and chronic respiratory ailments as in cystic fibrosis) suspected to have silent GER. An ideal oesophageal test should detect GER, establish a causal relationship between the event and disease, provide information about the nature and extent of reflux, detect the pathologic changes wrought by the disease and establish a differential diagnosis if any. This is a tall order and as expected no single test can provide all the information. Hence the tests need to be done in a judicious manner depending on the information required. This study has been the traditional choice; but it has several limitations. It lacks sensitivity and specificity. GER is a 24 hours diurnal event and any study that focuses on a brief period of time is certainly at a loss. As yet there is no universally standardized technique. Ideally the study should be done on a relatively relaxed and comfortably restrained supine infant. The infant is fed barium through a feeder with the head end slightly elevated. Adequate barium, comparable to a normal feed volume is ingested to fill the stomach. The infant should be supine now. During this period, judicious, intermittent fluoroscopy is utilized to observe the dynamics of swallowing, oesophageal transit and once the stomach is adequately full, for the occurrence of reflux (Fig. 7.9.3). Provocative measures to elicit reflux is best avoided as they do not represent a physiologic event. Clear fluid or water may be given to washout the oesophagus when needed, and to look for GER; as this can be considered to simulate a life event. Once that is done, passage of barium from the stomach to the proximal small bowel is observed. This is done to evaluate the duodenal ‘C’ loop and the DJ flexure to exclude malrotation and other obstructive pathologies. The study has to be as brief as possible as one is dealing with ionizing radiation. The upper GI series is not for just documenting GER but done to evaluate other causes of vomiting as it provides excellent anatomic information along with motor function.
7.9: Upper gastrointestinal abnormalities (typically seen in infants and young children)
Introduction
Method of examination
Contrast media
Oesophagogram/upper GI series
Oesophagus – normal features
Gastro-oesophageal reflux (GER)
The upper GI series
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


