The ureter is a tubular structure measuring up to 3 mm in diameter and 25 cm in length. It carries urine to the urinary bladder from the kidney and is entirely retroperitoneal in its course. It arises from the renal pelvis at the pelviureteric junction emptying distally into the urinary bladder at the vesicoureteric junction (VUJ) The inner cell layer of urothelium is surrounded by an outer smooth muscle layer which allows coordinated contraction and peristalsis hence the excreted contrast agent may not opacify the entire ureter.
In the past, plain radiographs of the abdomen and ultrasound were used for indirectly evaluating and imaging the ureters, in addition to visualizing and evaluating the kidneys and bladder.
Recently, computed tomographic (CT) urography has emerged as the imaging modality of choice for evaluating the ureters, as well as the kidneys, bladder. The urethra can also be evaluated.
A CT urography comprehensively evaluates the urinary tract, allows detailed assessment, as well as helps visualize the surrounding structures in the abdomen and pelvis. It is now the gold standard in evaluating patients with haematuria when a screening ultrasound is negative or shows equivocal results. It is also used in the initial staging and follow-up of patients with urothelial tumours.
The entire ureter may not be opacified on a single acquisition. Various methods to overcome this include good hydration prior to contrast administration, administration of a diuretic and imaging in the prone position. Of these, good hydration prior to contrast administration probably gives the best results.
Dual-energy CT urography allows a single contrast-enhanced acquisition phase. Virtual nonenhanced images are created thus reducing the radiation dose. The technique is limited by decreased sensitivity for small stones, noisy images and inaccurate attenuation values.
Ultrasound though easily available, cheap and having no radiation risk has the inherent problem of nonvisualization of ureters when normal in calibre. Also air-distended bowel loops interfere with visualization and assessment of ureters which are mild or moderately dilated.
Noncontrast MR urography can help visualize normal ureters though dilated ureters are better visualized and evaluated. Administration of a diuretic helps better ureteric visualization. A contrast MR urography with or without diuresis since it is three-dimensional, aids delineation of the ureters, their course and calibre and helps delineate or rule out intrinsic ureteric lesions as well as extrinsic causes of ureteric obstruction. Periureteric fat stranding if seen on CT or MR could be secondary to inflammation or infection.
Inflammatory and hyperplastic conditions of ureter
These are uncommon lesions of the ureter. They manifest as single or multiple filling defects. On CT urography they cannot be reliably distinguished from other causes of filling defects like tumours or blood clots, hence ureteroscopic evaluation is required.
Ureteritis
Infection or inflammation of the ureter results in ureteral thickening with associated enhancement and periureteral fat stranding.
Ureteritis can be seen in the setting of cystitis, pyelonephritis or pyonephrosis.
A few infections, such as tuberculosis, fungus and schistosomes may cause discrete filling defects.
In tuberculosis, the kidneys are involved before the ureter. Findings in the kidneys include papillary necrosis, parenchymal destruction and calcification.
The ureteric wall maybe thickened with focal nodular areas appearing as filling defects on CT. Figs. 10.14.1 and 10.14.2 depict imaging appearance of ureteritis in 2 different patients.
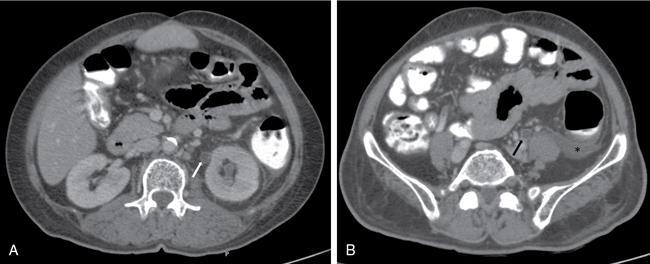
Fig. 10.14.1A case of left-sided ureteritis. CECT axial images at the level of proximal (A) and distal ureter (B) showing ureteric wall thickening on the left side (white arrow in A and black arrow in B). The patient also had left-sided pyelonephritis with thickening of left pararenal fascia and fluid along left paracolic gutter (asterisk).
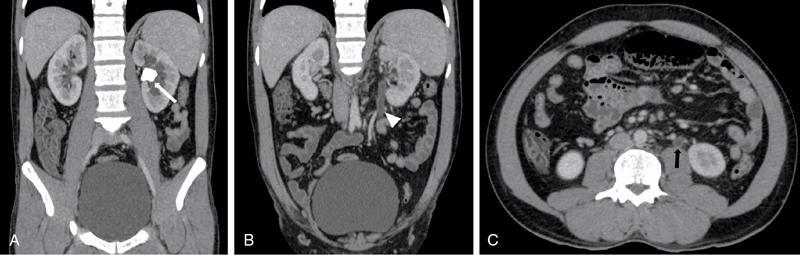
Fig. 10.14.2Ureteritis: Coronal post-contrast (A and B) and axial post- contrast (C) images in a 30-year-old patient with right flank pain, burning micturition and pus cells on routine Urine examination: Left pelvi-ureteric junction calculus (white arrow in A) is seen causing mild hydronephrosis. There was enhancing thickening of proximal ureteric wall on left side (white arrowhead in B and black arrow in C) with prominence of ureteric lumen without any distal filling defect.
Debris or sloughed papillae may also cause filling defects if associated papillary necrosis is present.
Strictures can occur at multiple levels, the common sites include the infundibula, renal pelvis, pelviureteric junction and the ureter. Ureteric strictures have a typical beaded appearance.
Fungal infections like candida and aspergillosis are common in immunocompromised patients. These can result in fungal balls or mycetomas which are seen as filling defects within the collecting system. These may contain air or calcifications. Rarely a urobezoar can be formed if the fungal ball extends into the ureter. This can cause obstruction.
Schistosoma haematobium is a parasite endemic in Africa and the Middle East. It lays its eggs in the wall of the urinary tract. Oedema and inflammation surrounding the eggs can create a nodular filling defect. Over time the eggs calcify causing mural calcifications seen on CT.
Ureter tuberculosis (discussed in genitourinary tuberculosis)
Ureteritis cystica results in multiple filling defects which may also be seen in a multifocal UCC. The ureter is not obstructed hence not dilated.
Fig. 10.14.3IVP image showing pyeloureteritis cystica: Multiple smooth oval to round lucent filling defects are seen in both ureters (white arrow and arrowhead) and in left renal pelvis (black arrow). (Source: Courtesy of Dr. Mukund Rahalkar.)
In polyureteritis cystica, multiple small cysts are seen in the ureteric wall. These are seen as multiple small filling defects in the proximal ureter; however, the fluid containing cysts are too small to sample and obtain density measurements. The filling defects are more numerous than those in multifocal urothelial carcinoma.
Amyloidosis
Amyloidosis comprises a variety of protein-folding disorders. Extracellular deposition of amyloid/protein aggregates in the tissues is seen in amyloidosis.
Amyloidosis can be either:
1. Localized: This comprises 10%–20% of cases of amyloidosis. Organs involved include skin, tongue, larynx, trachea and lungs. The nervous system, gastrointestinal tract and genitourinary tract may also be involved. Urothelial carcinoma is mimicked by localized amyloidosis affecting the urinary tract.
2. Systemic: It can be
(a) Primary systemic disease or,
(b) Secondary systemic disease.
Primary disease can be seen in association with:
I. Immune dyscrasias
II. Multiple myeloma
III. Waldenström’s macroglobulinemia
Secondary disease can be seen in association with:
I. Chronic inflammatory pathologies (e.g. rheumatoid arthritis, Crohn’s disease)
II. Tuberculosis
Clinical presentation: Patients may have:
I. Dysuria
II. Haematuria which is painless
III. Urinary colic and retention
Aetiology: The exact aetiology of this condition is not known. Local synthesis of amyloid and infiltration of monoclonal plasma cells are possible causes.
Common sites of involvement: Prostate and seminal vesicles are commonly affected. Bladder, renal pelvis, ureter and urethra can also be involved.
Primary amyloidosis of the ureter is very rare as compared to involvement of the prostate, seminal vesicles and urinary bladder. It is commoner in females and presents in the late sixth decade. It is typically unilateral and commonly affects the distal third of the ureter resulting in ureteral stricture and hydronephrosis.
Localized amyloidosis of the ureter usually is benign and carries a good prognosis. Systemic amyloidosis must be ruled out prior to treatment.
Imaging findings:
Ultrasound is used as an initial imaging modality followed by CT and MRI.
Both ultrasound and intravenous urography (IVU) can reveal hydronephrosis.
Computed tomography reveals nonspecific diffuse thickening of ureteral walls with calcification.
Differential diagnosis would include:
I. Urothelial carcinoma
II. Tuberculosis
III. Schistosomiasis
IV. Haematoma
On MRI localized ureteric involvement is seen as a hypointense lesion on T2-weighted images without mass effect. This helps differentiate it from a carcinoma.
Urine cytology does not differentiate amyloidosis from urothelial carcinoma, because many of the amyloid deposits are subendothelial in location. Hence, cytology has a limited value (50% sensitivity for urothelial carcinoma).
Biopsy is diagnostic as Congo-red staining of the amyloid produces the classical appearance of apple-green birefringence under light microscopy with polarized light.
The type of amyloid protein may be determined with the help of treatment of the amyloid sample with potassium permanganate. Further information about the protein components of the amyloid may be provided by immunohistochemistry or mass spectroscopy.
Treatment: Systemic amyloidosis must be ruled out prior to treatment. This maybe a result of multiple myeloma, Hodgkin lymphoma and renal cell carcinoma. Serum and urine electrophoresis, chest radiography and if appropriate, rectal biopsy or fine needle aspiration of subcutaneous fat can help exclude systemic amyloidosis.
Ureteral stricture
Ureteral stricture is diagnosed when there is a fixed obstruction with proximal dilatation. A physiological narrowing should be excluded before diagnosing a stricture. Physiological narrowing manifests as focal narrowing or abrupt kink and characteristically does not have any proximal dilatation. Common sites for physiological narrowing include pelviureteric junction, pelvic brim and vesicoureteric junction. The length of the stricture and its location should be described in any radiological report for guiding appropriate management. While IVU is adequate for initial diagnosis of stricture, cross-sectional imaging maybe required to determine the underlying cause. Strictures may manifest as pure ureteral narrowing without any ureteral wall thickening or periureteral abnormalities. Secondary narrowing of ureter due to extrinsic compression (either due to local inflammatory pathology or any adjacent neoplasm) is readily diagnosed on CT or MR and should be ruled out before planning any urological intervention. Causes of ureteral stricture are enlisted in Box 10.14.1.
2. Encasement by an adjacent tumour (e.g. cervix, colon, lymphoma, retroperitoneal metastasis)
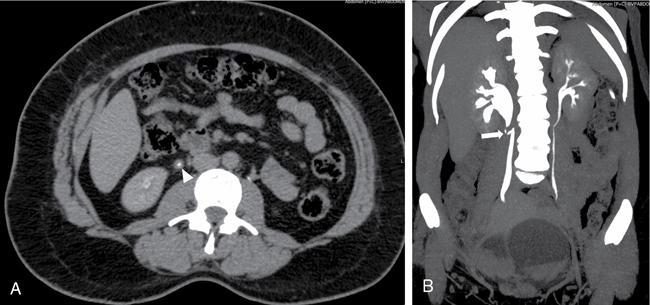
Fig. 10.14.4Benign ureteric stricture: CT Urography study of a 36-year-old female who complained of right lumbar pain. Axial image in excretory phase (A) shows inflammatory thickening of the proximal right ureter (white arrowhead). Coronal MIP image (B) shows inflammatory thickening and kinking of proximal right ureter (white arrow) causing moderate hydronephrosis.
Malakoplakia (discussed in infections)
This is seen on imaging as multiple nodules or polypoid lesions which are indistinguishable from multifocal urothelial carcinoma.
Periureteral diseases
Retroperitoneal pathologies may affect the ureter secondarily, compressing or encasing the ureter resulting in complications like hydronephrosis, obstructive uropathy and urinary tract infection.
Periureteric haematoma or urinoma
Periureteric and perirenal haematoma
Introduction
Haemorrhage around the kidney and ureter is common in posttraumatic cases similar to urinoma. Postoperative procedures can also result in haemorrhage. Spontaneous haemorrhage can occur, though uncommon. It can be a life-threatening condition. It can be subcapsular, perirenal haematoma or extend across the midline in the retroperitoneum.
Aetiology
Posttraumatic and postoperative causes are similar to that of urinoma. Postbiopsy renal pseudo aneurysms and bleed are known causes. Spontaneous haemorrhage can be due to tumours (angiomyolipoma more common than renal cell carcinoma), vascular causes, infection and unknown causes. Metastasis and antiplatelet agents are also described as cause for spontaneous retroperitoneal haemorrhage around the ureter.
Clinical features are usually related to trauma.
Imaging
Plain films and IVU are now rarely used for the diagnosis of haematoma. Plain films are useful in diagnosing bony fractures, in cases of traumatic haemorrhage.
Ultrasound shows cystic collection with internal echoes in it. However, it can mistake a haematoma for a solid mass due to the presence of echoes in it. In cases of angiomyolipoma, it can show an echogenic renal lesion as a cause for haemorrhage. However, it is very useful for follow-up of cases with haematoma.
CT with contrast and delayed images is the mainstay for diagnosis in majority of cases. In cases of trauma, it shows associated renal injury signs. The density of the collection on CT suggests it as haematoma. It can also tell about the cause for haemorrhage-like presence of fat in angiomyolipoma or a renal tumour causing haematoma. CT may not find a cause in cases of vascular causes and anticoagulation bleeds.
Angiography is necessary in diagnosis of vascular causes like polyarteritis nodosa (PAN). Findings in PAN can be vascular aneurysms and stenosis of nodules.
Urinoma
Introduction
A urinoma is loculated collection of urine outside the pelvicalyceal system. It can be traumatic, postoperative or spontaneous in the presence of obstruction. IVU was used to diagnose this condition in the past. However, after the advent of ultrasound and CT, they form the mainstay in diagnosis and location of the leak.
CT with delayed images is the most important imaging technique used to diagnose and locate the site of leak. Rarely antegrade and retrograde pyelography or scintigraphy maybe required in the diagnosis of the site of leak.
The extravasated urine causes inflammatory response. Deposition of fibrin and collagen tissue causes loculation resulting in urinoma formation.
The leaked urine usually lies in subcapsular or perirenal space. The collection can extend across midline in the retroperitoneum. Rarely, it can cross the diaphragm and extend into the mediastinum and pleural space. Extension in the thigh, pelvis, scrotum and perineum is also described. Intraperitoneal leak is usually secondary to trauma. Rarely bilateral urinomas are also described in literature.
Aetiology
Traumatic leaks are usually associated with renal or other retroperitoneal trauma. Causes of obstruction include posterior urethral valves in neonates, calculi, prostatic hypertrophy and tumours in adults. Bladder or ureteric cancers, metastasis or ovarian carcinomas can also rarely result in urinoma formation.
Unlike renal causes, ureteral causes for urinoma formation are mostly iatrogenic, following postsurgical antegrade or retrograde pyelography in patients who have undergone procedures like urinary diversion, renal transplantation.
Clinical features include increasing abdominal girth following trauma and postoperative fever due to infection.
Only gold members can continue reading. Log In or Register to continue