Aniruddha Joshi URETHRAL DIVERTICULUM (URETHROCELES) Urethroceles are focal outpoching of urethra. Ultrasonography (US) and MRI have improved our diagnostic ability and understanding of the disease. Women especially those with stress incontinence are affected more frequently than men. Most of the women are between the ages of 30 and 50 years. These patients commonly present with nonspecific clinical symptoms – dysuria, postvoid dribbling, dyspareunia, frequency/urgency, recurrent haematuria, stress incontinence. Some of the patients may develop stones within the diverticulum. Repeated infection and irritation predispose to malignant transformation of the lining urothelium. Urethral diverticulum is an epithelized outpouchings of the urethral lumen into the surrounding periurethral connective tissue. Aetiology of the urethral diverticulum is unknown. Current hypothesis states that repeated infection and obstruction of the periurethral and paraurethral glands (Skene’s gland) results in formation of cyst/abscess. At some point these rupture into the urethral lumen and connect to urethra via a neck or ostia. These outpouchings may be simple in nature, may partially encircle the urethra (saddlebag), or may completely envelop the urethra. Sometimes, they extend proximally beneath the bladder neck and trigonal area. Complicated anatomical patterns, however, may exist with multiple ostia. Iatrogenic damage to the urethra may also play a role in formation of the diverticulum. Voiding cystourethrography and double-balloon catheter urethrography (DBU) were used to be considered investigations of choice (Fig. 10.15.1.1). Transabdominal, transvaginal, transperineal or transluminal USG techniques have been described with the patient in the dorsal lithotomy or supine position. These techniques are operator-dependent leading to drawback in diagnosing of urethral. USG provided particular benefit in differentiating a septated urethral diverticulum from multiple urethral diverticula compared with MRI. Poor soft tissue contrast causes limitation to the conventional contrast-enhanced CT. Urethral diverticulum may be visualized at as a hypodense mass with wall thickening and enhancement at the level of the pubic symphysis. However, urethral calculi in the dependent portion of diverticula can be reliably shown. Recently MRI has become the imaging study of and is strongly advocated before performing any surgery. Diverticuli appear T1 hypointense and T2 hyperintense. IV gadolinium can be administered for detection of inflammation, infection or malignancy (Fig. 10.15.1.2). The differential diagnosis of urethral diverticulum includes: vaginal wall cysts, leiomyoma, Skene’s gland abnormalities, Gartner’s duct abnormalities, urethral prolapse, ectopic ureterocele urethral diverticular adenocarcinoma and urethral caruncle. URETHRAL TRAUMA Urethral traumatic injuries may be of blunt, penetrating or iatrogenic types. Other uncommon causes of injuries are penile fracture and injuries resulting from pancreas transplantation. Diagnosis and extent of the urethral injuries require high-quality imaging for effective treatment planning. Male urethral injuries are much more common than female urethra. In clinical setting of trauma, blood at the external urethral meatus, vaginal introitus and haematuria may be seen, but these are unreliable signs. Complete urethral disruption, there may be overdistended bladder with inability to void, perineal ecchymosis and on DRE impalpable/high riding prostate. Dysuria, urinary urgency and suprapubic discomfort can ensue in the chronic stages of incomplete urethral injury due to complicating strictures. Urethral trauma is associated with blunt trauma, penetrating or iatrogenic types. Most commonly associated with motor vehicle accidents. Other less common causes are penile fracture, urinary extravasation in pancreas transplantation, instrumental childbirth. Urethral traumatic injuries occur commonly associated with motor vehicle accidents. Depending on location, these can be anterior or posterior urethral injury. Anterior urethral injuries are associated with direct blow to perineum, straddle injury, penetrating traumas, penile fracture and iatrogenic. Bulbous urethra is most commonly injured in this. Posterior urethral injury is far more common. These are associated with road traffic accident and fall from a height. Posterior urethra is in close relation to the pubic bones and the puboprostatic ligaments. Urethra is also susceptible to injury by the displaced fracture fragments. The distal membranous urethra is especially at risk. Female urethral injury is rare due to short length, internal location and less rigid attachment of the urethra to the adjacent pubic bone. And in severe pelvic trauma during road traffic accidents, there can be bladder neck injuries extending into the urethra. Iatrogenic traumas may result in injury at any level of the urethra and are seen as a consequence of urological interventions, surgery or radiotherapy. In acute traumatic setting, any visceral/vascular injury should be managed to achieve haemodynamic stability. Patients with clinical signs indicative of urethral injury should be considered for immediate urethrography. On imaging if urethra appears intact, catheter may be inserted. If there is urethral or bladder injury, a suprapubic catheter should be inserted and later to be posted for surgery. Patients without clinical signs of urethral injury do not require immediate urethral imaging. If inadvertently blind catherization is done, it may complicate haemorrhage or increase the degree of urethral tear. On plain radiography, presence of pelvic fractures with disalignment should raise suspicion for urethral injury. Fractures of ischiopubic rami or separation of the symphysis pubis is more indicative of urethral injury. It is the standard diagnostic investigation for evaluation of a male urethral injury. Ideally ascending (or retrograde) and descending (or antegrade) urethrohraphic studies should be performed for evaluation of anterior and posterior urethra. And on follow-up imaging retrograde imaging is required. In traumatic setting, patient mobility and proper imaging techniques are not always possible. In these cases, foam cushions may be placed underneath the patient to help maintain that position, the tube may be rotated to a 30-degree left anterior oblique angulation or the table may be elevated to a 45-degree angle during voiding with a footrest. Urethrogram allows identification of the site of injury and extent of any injury. Any extravasation outside the urethra is pathognomonic for urethral injury. Prostatomembranous urethra is commonly injured just above the urogenital diaphragm. On excretory urography, high-riding urinary bladder is seen due to disruption of puboprostatic ligaments and haematoma in the pelvis. Extravasation of contrast extravasation can be seen adjacent to the posterior urethra and sometimes into the pelvic extraperitoneal space (Fig. 10.15.2.1).
10.15: Urethra
Introduction
Epidemiology
Clinical features
Pathogenesis
Imaging
Urethrography

Ultrasound
CT
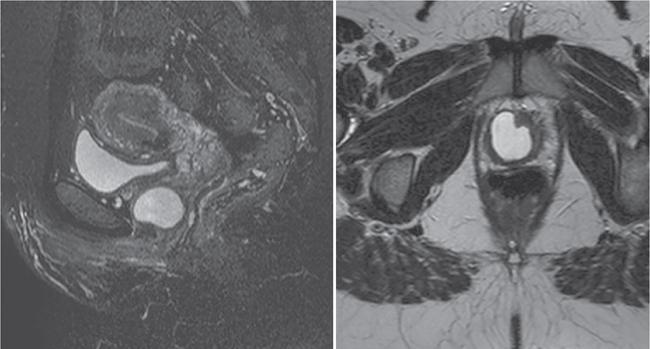
MRI
Differential diagnosis
Epidemiology
Clinical features
Aetiology
Pathology
Imaging
Plain film radiography
Urethrography
Posterior urethral injuries

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


