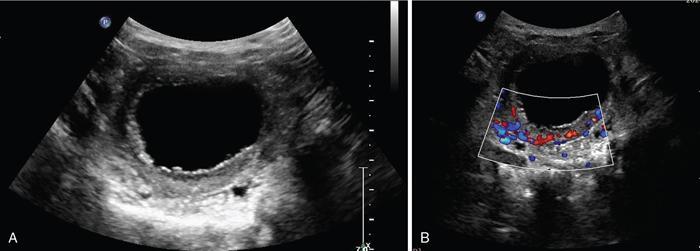
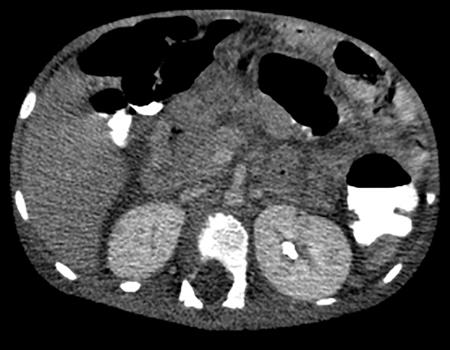
Anmol Bhatia, Ajay Prashanth Dsouza, Kushaljit Singh Sodhi Urinary tract infection (UTI) is a common cause of febrile illness in children, second only to respiratory tract infections. The incidence before 14 years of age ranges from 3%–10% in girls and 1%–3% in boys; however, the incidence is more in boys during infancy. The clinical spectrum in increasing order of severity ranges from asymptomatic bacteriuria and cystitis to acute pyelonephritis and septicemia. Urinary tract anomalies, prematurity, indwelling urinary catheters, lack of circumcision in boys and high-grade vesicoureteral reflux (VUR) are some of the common predisposing factors. Although the clinical outcome is good in most patients, a few may develop long-term complications like hypertension, chronic renal insufficiency and end-stage renal disease. Given the poor localizing signs and the dreaded complications, a high degree of clinical suspicion, prompt diagnosis and treatment and tailored follow-up play pivotal role in management of these patients. Urine culture is the most important tool to establish the diagnosis and identify the causal pathogen, Escherichia coli being the most commonly isolated bacteria. Midstream clean catch urine sample is used in toilet-trained children while the sample is often obtained by suprapubic aspiration or transurethral catheterization in younger age group. A colony count of >105 CFU/mL of a single species in a midstream clean catch sample is confirmatory. Although imaging can aid in the diagnosis of an ongoing UTI, the main role lies in identifying the associated urinary tract abnormalities and also to look for the extent of consequent renal insult. Some of the common anatomic abnormalities predisposing to recurrent and complicated infections include VUR, congenital pelviureteric junction (PUJ) obstruction, ureterocoele, posterior urethral valve, ureteral duplication and neurogenic bladder. The imaging modalities commonly used in children are ultrasound (US), which helps in detection of structural anomalies, hydroureteronephrosis, urinary tract stones and renal scars; voiding cystouretherography (VCUG) for detecting VUR and 99mTc-labelled dimercaptosuccinic acid (DMSA) scans to look for renal scars. US is often used as the first-line imaging modality because of its easy availability, low cost, non-invasiveness and lack of ionizing radiation. UTI, when confined to the lower genitourinary tract, frequently called as cystitis, reveals diffuse bladder wall thickening (Fig. 10.8.1A) with hazy margins on grey-scale US, which may show increased vascularity on Doppler (Fig. 10.8.1B). Floating echoes in the urine are commonly seen. The distal ureter may also be dilated and show mural thickening. Since UTI confined to bladder is mostly uncomplicated, it does not usually warrant a further imaging workup. However, in cases of severe bladder trabeculations, unilateral gaping ureteral ostium, open bladder neck, follow-up for bladder outlet obstruction, dysfunction or VUR may be indicated after the acute infection settles. Inflammatory response to the infection leads to swelling and decreased perfusion in renal parenchyma. Findings on intravenous urography (IVU) include renal enlargement, a diffuse or patchy striated nephrogram with delayed opacification and effacement of pelvicalyceal system. On renal US, diffuse or localized renal enlargement may be the only finding. Other typical findings include altered parenchymal echotexture, usually hypoechoic (Fig. 10.8.2) but may be hyperechoic, along with poor corticomedullary differentiation. Colour or power Doppler study reveals reduced vascularity. On 99mTc DMSA or glucoheptonate scans, photopenic defects due to reduced accumulation of renal cortical tracers are seen. The defects may be solitary, multiple or may involve the entire kidney giving a mottled appearance. DMSA renal scintigraphy with a sensitivity of 99.9% is the imaging modailty of choice for diagnosing acute pyelonephritis (APN). Among the patients with UTI, 50%–91% show defects on nuclear scans, suggestive of acute pyelonephritis. When both VUR and APN are present, scintigraphy is abnormal in 79%–86% of children. Permanent scars are known to occur in 38%–57% of children diagnosed with APN on nuclear scan, not withstanding the grade of VUR. 99mTc DMSA scan is the imaging modality of choice for detection of renal scars and they also appear as photopenic defects; however, the temporal course of study helps to differentiate it from APN. Thus, follow-up scanning at 3–6 months may be suggested to detect if the kidney has healed or scarred. CECT reveals striated nephrogram along with multiple wedge-shaped or round hypoenhancing areas with apices directed towards calyces (Fig. 10.8.3). Perinephric fat stranding may also be seen. MRI reveals wedge-shaped or round, T2 hyperintense lesions with decreased signal on inversion recovery sequences. And similar to CECT, striated nephrogram and inflammatory changes in perinephric fat may be demonstrated. MRI can also help in detection of renal scars. Despite it being a radiation-free modality with utility in poor renal function, MRI is less often used due to limited availability, higher cost, longer scan times and need for prolonged sedation. Acute focal bacterial nephritis is a localized or segmental form of acute pyelonephritis, also known as acute lobar nephronia, usually affecting only a renal pole or one moiety in a duplex kidney. It appears as an ill-defined, poorly marginated mass in contrast to renal abscess which is relatively well-defined, surrounded by enhancing walls (Fig. 10.8.4). The mass is usually hypoechoic on USG with low-level internal echoes and shows reduced vascularity on Doppler. CECT shows ill-defined or wedge-shaped hypodense areas which correspond to focal photopenic defects on nuclear scans.
10.8: Urinary tract infections (including vesicoureteric reflux and neurogenic bladder)
Introduction
Role of imaging in UTI
Imaging in cystitis
Imaging findings in acute pyelonephritis


Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


