Uterine Carcinoma
Todd M. Blodgett, MD
Alex Ryan, MD
Sanjay Paidisetty, BS
Key Facts
Imaging Findings
Primary endometrial cancer: Thickened endometrium on CT with intense FDG activity on PET, correlating with mass
MR/CT used to evaluate disease extension and provide information for treatment planning, ± ultrasound
FDG PET for staging, restaging, early detection, evaluating response to therapy
Signs of metastatic disease on PET/CT: Lymphadenopathy with increased FDG, abdominal/distant metastases
PET/CT useful for anatomic and functional localization of sites of recurrence
Significant nonmalignant uptake in younger patients who are menstruating
Sensitivity of PET alone (87%) or plus MR or CT (91%) is higher than MR or CT alone (˜ 67% in overall lesion detection)
PET most useful for detecting distant metastases
Top Differential Diagnoses
Uterine Leiomyoma
Endometrial Hyperplasia
Endometrial Polyp
Cervical Cancer
Endometrial Sarcoma
Diagnostic Checklist
MR or CT for extent of primary tumor
PET/CT for optimal staging
Note benign causes of increased FDG activity in endometrium (e.g., menstruation)
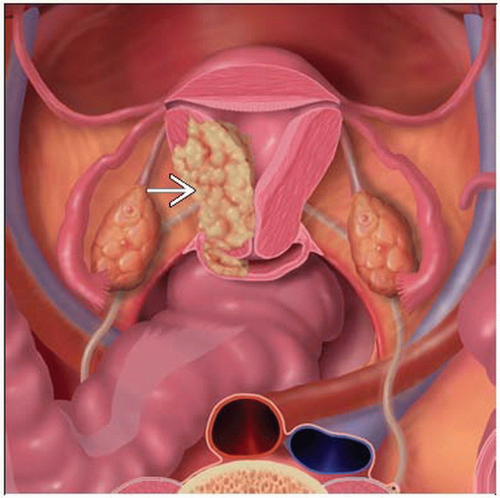 Graphic shows a representation of uterine body carcinoma  . . |
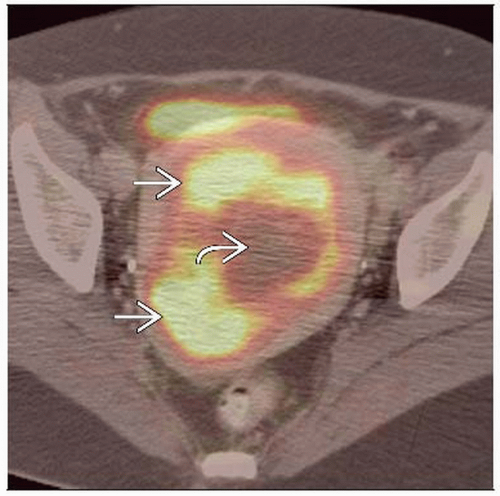 Axial fused PET/CT shows an enlarged uterus with circumferential FDG activity  and central necrosis and central necrosis  in this patient with uterine leiomyosarcoma. in this patient with uterine leiomyosarcoma. |
TERMINOLOGY
Abbreviations and Synonyms
Endometrial carcinoma, uterine sarcoma, uterine carcinosarcoma, leiomyosarcoma
Definitions
Malignancy of uterine endometrium or uterine body
Most common type is endometrioid adenocarcinoma
IMAGING FINDINGS
General Features
Best diagnostic clue
Primary endometrial cancer
Thickened endometrium on CT
Intense FDG activity on PET corresponding to lesion
FDG uptake in metastatic sites
Lymphadenopathy
Abdominal and distant metastases
Location
Usually glandular component of superior endometrium
May spread within endo-/myometrium and from fundus toward isthmus and cervix
May arise within an endometrial polyp
Imaging Recommendations
Best imaging tool
CT/MR
Evaluate disease extension
Provide information for treatment planning
Detect lymph node metastases; 18-66% sensitivity and 73-99% specificity
Limited in recurrent disease due to anatomic distortion 2° surgery and radiation
FDG PET
For staging, restaging, early detection, and evaluating response to therapy
Incorporation of FDG PET into post-therapy surveillance shown to influence treatment in up to 20% of patients
Particularly useful for asymptomatic disease
PET/CT useful for anatomic and functional localization of sites of recurrence
Protocol advice
Oral contrast agent for CT
Helps better delineate normal bowel activity
Demonstrates pathologic intra-abdominal activity (peritoneal implants)
IV contrast
Differentiates small lymph nodes from vessels, intestine, or the ureter
Correctly detects small liver metastases, small peritoneal dissemination, and local recurrence at the vagina
CT Findings
Inconsistent depiction of endometrium and endometrial thickness
Findings associated with endometrial carcinoma are nonspecific and similar to other conditions
Uterine cancer and normal endometrium are often indistinguishable on nonenhanced CT
May see diffuse thickening, discrete mass, or polypoid mass within endometrial cavity
Cavity may be expanded with fluid
Mass may be of uniform or heterogeneous attenuation
Usually poorly enhancing relative to myometrium
Variable areas of contrast enhancement
IV contrast also aids in evaluating local invasion by increasing conspicuity of tumor
Invasion of myometrium suggested by irregular tumor-myometrium border
CT limited in ability to delineate deep myometrial invasion and cervical involvement
CT reasonably sensitive for lymphadenopathy and distant metastases
Size cutoff for suspicion of malignancy > 8-10 mm in short axis
MR Findings
T1WI
Endometrium and myometrium have similar signal intensity and cannot readily be distinguished
T2WI
Endometrium appears as central zone of high signal intensity
Myometrium depicted as zone of low signal intensity at its inner aspect and a wider zone of intermediate signal intensity at its outer aspect
Endometrial thickness varies in menstruating women from 4 mm in early proliferative phase to 13 mm in late secretory phase
Nuclear Medicine Findings
General
Sensitivity of PET alone (87%) or plus MR or CT (91%) is higher than MR or CT alone (˜ 67% in overall lesion detection)
PET has 89% PPV and 91% NPV in patients with endometrial cancer; 87.5% and 97.5% for uterine sarcoma
Lesion size-related sensitivity
< 4 mm: 16.7%
5-9 mm: 66.7%
Mean SUV of true positive lesions in one study
13 for central pelvic lesions
11 for metastases
False positives
Normal cycle variation of FDG activity in endometrium
Significant nonmalignant uptake in younger patients who are menstruating
Bone fracture
Post-operative changes
Staging
Primary benefit of FDG PET is improved staging of distant metastatic diseaseRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


