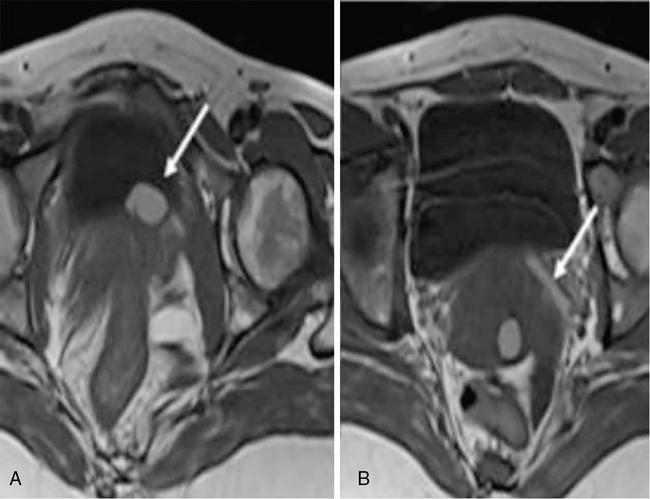
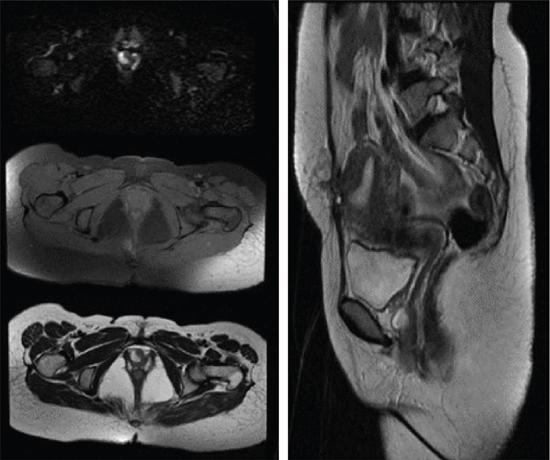
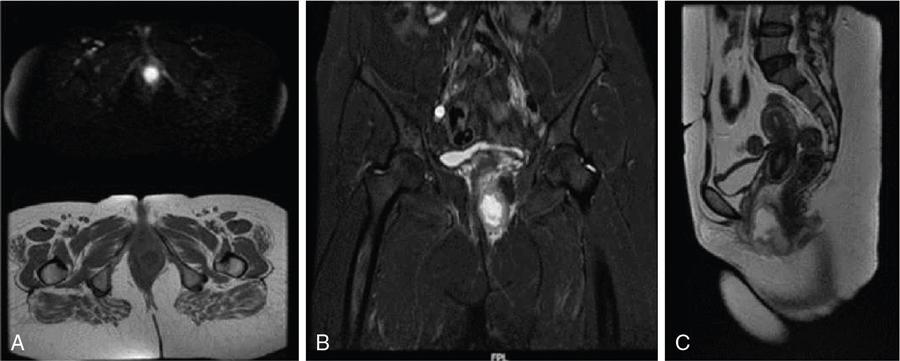
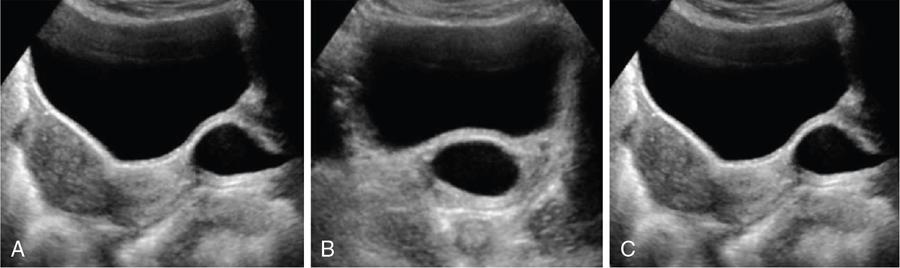
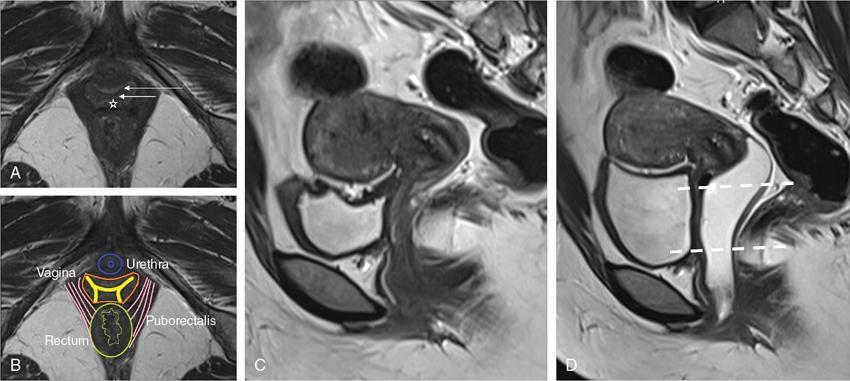
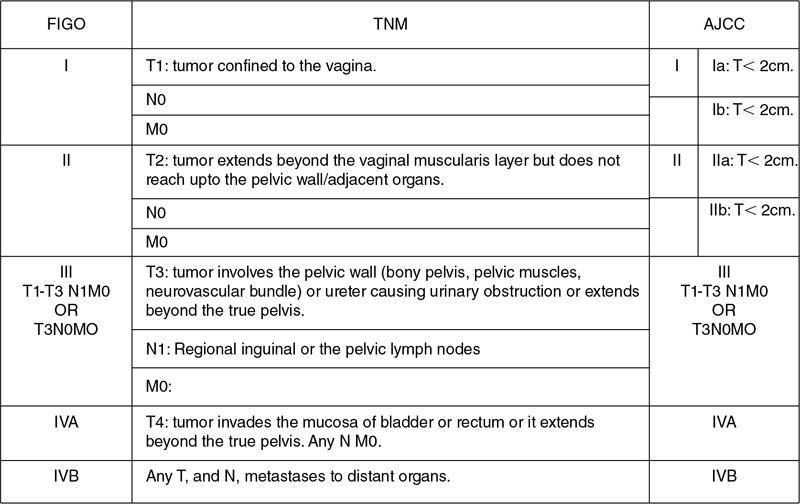
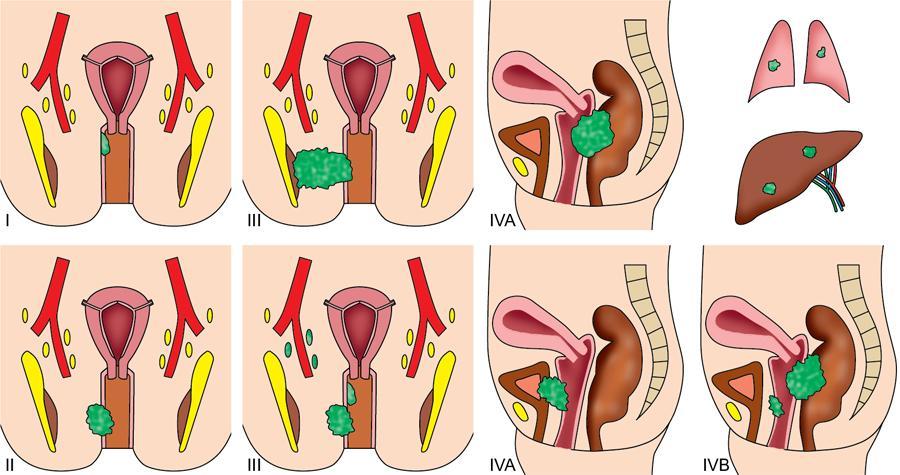
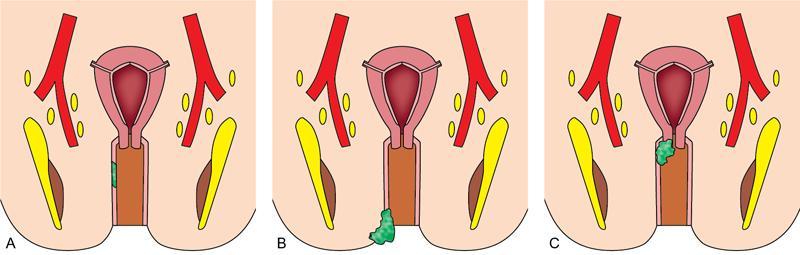
VAGINAL CYSTS Sumeena The vagina is a fibromuscular sheath. Vagina extends from uterus to the vulvar vestibule. The vagina is located in the middle compartment of the pelvis and it is related anteriorly to bladder and urethra, posteriorly to lower rectum and anal canal. The length of vagina ranges from 4 to 12 cm. The posterior wall of vagina is longer and it ends in posterior fornix; the anterior wall is shorter and ends in the anterior fornix. The wall of vagina is composed of three layers: (a) The mucosa consists of nonkeratinized stratified squamous epithelium without glands and its hormone sensitive layer; (b) the muscularis made up of connective tissues and smooth muscle; and (c) the adventitia, which is fascia that connects the vagina to the surrounding pelvic structures and maintains support. The prevalence of vaginal cysts is estimated to be less than 1%. They typically present in the age of 30–40s. Their origin may be Müllerian, Wolffian, squamous or urogenital. Risk factors for vaginal cysts: The vagina may be underevaluated due to probe positioning in routine pelvic US and due to poor vaginal tissue characterization in CT examinations. Though MR imaging provides good tissue characterization, we must focus on the vaginal region to identify any incidental findings. The strengths and limitations of each imaging modality must be understood in assessing the vagina. US is the first-line imaging modality since it is readily available, cost-effective, high resolution and no ionizing radiation. Limitations include operator dependence and patient obesity. The major limitation with transabdominal approach is that the upper portion of the vagina is seen well; the inferior aspect of the vagina is obscured due to shadowing from the pubic symphysis. Limitation with transvaginal US is that the transducer is typically placed in the anterior or posterior fornix which bypasses the perineum and vagina. US imaging needs methodic evaluation performed from introitus to the fornices and include transabdominal, transvaginal and translabial approaches. Due to the poor vaginal tissue characterization and ionizing radiation, CT is usually not indicated for evaluation of the female pelvis. When US is inconclusive, pelvic MR imaging is recommended. The vaginal wall anatomy is best imaged with T2-weighted sequences. The vaginal mucosa has high signal intensity, circular and longitudinal muscle layers have intermediate signal intensity. Embryonic Traumatic Epithelial inclusion cyst/epidermal inclusion cyst/squamous inclusion cyst Skene’s duct cysts Urethral diverticulum Infective Filariasis Vaginitis emphysematosa Epidermoid cyst Sebeceous cyst Endometriotic cyst Ciliated cyst Paraurethral mass Rare Lymphangioma Postradiation Haematocolpos Rectocele and cystocele Prolapsed ectopic ureterocele Large nabothian cyst, tunnel cluster cysts Adenoma malignum Most common type of vaginal cysts, almost up to 40% of cystic masses. As Müllerian epithelial tissue can present anywhere in the vaginal wall, the cysts can also be found anywhere within the vaginal walls. Most common location is along the anterolateral aspect of the vagina. Müllerian cysts present as small, midline cystic masses, with no symptoms and require no treatment. Symptomatic vaginal cysts are treated by excision. The entire cyst wall must be removed to prevent recurrence. Adenocarcinoma can arise in a Müllerian vaginal cyst. The epithelium of Gartner’s cysts is devoid of cytoplasmic mucicarmine and PAS-positive material, in contrast to the epithelium of Müllerian cysts. MRI – Gold standard. Mucus secretion is a unique feature of Müllerian cysts and shows heterogeneous T2 signal. Extent of the cyst, surrounding structures are better evaluated in MRI prior to surgery. Incomplete regression of Wolffian ducts leads to the development of Gartner duct cysts. They are usually noted in the upper anterolateral wall of the vagina above the inferior border of the pubic symphysis. Typically less than 2 cm. When these cysts are large enough, they can compress the urethra causing urinary symptoms. It can also be associated with abnormalities of the metanephric urinary system such as an ectopic ureter, unilateral renal agenesis and renal hypoplasia. USG: Anechoic structure in the upper vagina; transvaginal US provides better differentiation than the transabdominal approach. Fig. 11.19.1.1; T2-axial image shows hyperintense cystic lesions, one in posterior fornix and another one in anterior aspect of upper vagina. Both the lesions are above the level of pubic symphysis. Fig. 11.19.1.2; T2-sagittal image shows hyperintense cystic lesions, one in posterior fornix and another one in anterior aspect of upper vagina. Both the lesions are above the level of pubic symphysis. Bartholin glands are commonly located posterolateral to the vaginal introitus and medial to the labia minora. The obstruction of the gland’s duct either by a stone or a stenosis, which may be caused by prior infection or trauma, leads to Bartholin gland cysts. Cysts are typically round and unilocular, seen at or below the level of the pubic symphysis, usually asymptomatic. This is most apparent on coronal plane imaging. USG: Bartholin gland cysts can be imaged by a transperineal approach. Although these cysts are usually asymptomatic, occasional infection may necessitate drainage of the cysts (Fig. 11.19.1.3). Bartholin gland duct can be obstructed due to stone or stenosis, later which can become infected. The Bartholin’s gland abscess size ranges from 2 to 8 cm with an average of 3 to 4 cm. Antibiotics with or without surgical drainage is the treatment. Marsupialization may be needed in recurrent conditions. USG-complex cystic hypoechoic to anechoic lesions increased throughout transmission. Colour Doppler may show peripheral hyperaemia. Spectral flow – low resistance arterial flow. MRI-T2: Tends to show heterogeneous signal T1 C+ (Gd): pericystic enhancement may be seen (Fig. 11.19.1.4). Vaginal inclusion cysts – also known as epidermal inclusion cysts, most commonly are seen in the distal posterior or lateral vaginal wall at sites of previous trauma or surgery. Inclusion cysts are lined by a stratified squamous epithelium and contain keratinous material. Symptomatic cyst needs treatment. The treatment of choice for symptomatic cysts is marsupialization. MRI-DWI shows restriction (Fig. 11.19.1.5). Skene glands are paired structures in periurethral location near external urethral meatus with ducts draining into the urethra. Skene gland cysts can cause UTI or urethral obstruction. They are distinguished from urethral diverticulum, which are usually midurethral. In T2-weighted images, Skene duct cysts seen as round or oval hyperintense lesions just lateral to the external urethral meatus. MRI:T1 hyperintense due to proteinaceous material. T2 hyperintense. Fluid–fluid level if complicated with debris or haemorrhage (Fig. 11.19.1.6). It may be congenital or result from infection or obstruction. In females, diverticula commonly extends from the posterolateral wall of the mid-portion of the urethra. During voiding cystourethrography (VCUG), they are seen best on postvoid images. Transrectal US shows a cystic mass in proximity to the urethra and it will be seen anterior to the vagina. Lack of radiation and capacity to differentiate solid from cystic masses is the advantage of US over CT. CT shows a periurethral lesion with low attenuation. MRI shows T1 hypointense and T2 hyperintense fluid signal intensity. Postcontrast imaging with gadolinium is used to evaluate infection or inflammation. Adenoma malignum of the cervix is a rare variant of cervical mucinous adenocarcinoma. VAGINAL MALIGNANCIES Rupa Renganathan, Suchana Kushvaha The primary vaginal carcinoma is a very rare gynaecological malignancy and accounts for 2%–3% of genital tract malignancies and 10% of all vaginal malignancies. It is defined as a cancer found in the vagina without histological or clinical evidence of cervical or vulvar malignancy and without previous history of treatment of cancers in the last five years. The commonest primary carcinoma is squamous carcinoma, and other rare primaries are adenocarcinoma, melanoma and sarcomas. The secondaries in the vagina are much more common than the primary and account for more than 80% of vaginal malignancies. Primary vaginal carcinoma is common in elderly, however, seen in the younger women when associated with human papillomavirus (HPV 16 and 18). Vaginal carcinomas are staged based on FIGO classification. Management of the cancer is usually based on the stage of the disease and the histological subtypes. Vagina is an elongated fibromuscular structure connecting the uterus with the vulva. It is approximately 7–9 cm long. The long axis is oriented 90 degrees to the uterine axis and its upper part is oriented almost horizontally and in plane with the pelvic floor. It is lined by the nonkeratinizing stratified squamous epithelium. It has anterior, posterior and lateral walls. The upper portion of vagina is invaginated by the cervix such that a space is created between its walls and the cervix called fornices. The posterior fornix is deeper than the anterior fornix. Anterior wall is separated from the bladder base and the urethra by the anterior vesicovaginal septum while the posterior wall is separated from the rectum by rectovaginal septum. The posterior fornix is covered with the peritoneal reflection that forms the Pouch of Douglas. It is supplied by the vaginal arteries, originating from the internal iliac artery and branches of uterine, middle rectal and inferior vesical arteries. There is considerable overlap in the lymphatics between the various parts of vagina. The upper two-thirds of the vagina drain into the pelvic lymph nodes that include external, internal and common iliac groups and the lower third into the superficial inguinal and femoral lymph nodes. The posterior vaginal wall also drains into the perirectal lymph nodes. MRI is the standard imaging modality for local staging of cancers and also for assessment of treatment response and surveillance due to superior soft tissue resolution, multiplanar capability. In a relaxed state, it is seen as a ‘H’ shaped structure posterior to urethra with the anterior and posterior walls being opposed to each other. The vaginal lumen may have secretions or blood-causing distention of its lumen. The anatomy of the vagina is best depicted on T2w images where three layers of its wall can be distinguished in a nondistended state. The mucosa is T2 hyperintense with a hypointense submucosal and muscularis layer beneath it. It is surrounded by adventitia which is hyperintense due to the venous plexus (Fig. 11.19.2.1A and B). For accurate staging purposes, vagina should be distended with ultrasound gel with the help of a syringe and infant feeding tube (Fig. 11.19.2.1C and D). Before inserting gel, patient consent must be taken and her marital status should be enquired. Care must be taken that air is not insufflated while introducing the jelly. Jelly can also be introduced in patients other than carcinoma vagina in cases where vaginal involvement is suspected in other malignancies. After adequate distention, the walls get separated and the fornices are better delineated. For staging purposes, the vagina is divided into three parts. The upper one-third lies above the level of the bladder base and includes the fornices. The middle one-third is opposite to the bladder base and the lower one-third opposite to the urethra (Fig. 11.19.2.1D). Ultrasound owing to its limited field of view and inaccurate staging is not used for imaging of vaginal pathologies. CT has poor contrast resolution and is used only for lymph nodes staging in known patients of vaginal malignancy. PET CT has the advantage in that it combines both the functional and anatomical information about the tumour. While performing PET for the gynaecological malignancies, general measures to reduce bladder activity, like Foley’s catheterization, IV hydration and diuretic administration, are adapted and the image acquisition is done from the pelvis cranially. The advantage of PET beyond providing functional information is that it provides information about distant metastases. The presence of nodal metastases in patients with vaginal cancers portends a poor prognosis and alters the management. In a study by Christensen et al., PET CT was found to be more sensitive and carried greater negative predictive value as compared to MRI for detection of lymph nodes. However, commonly seen inflammatory and the reactive lymph nodes may show uptake. Node biopsy or excision is mandatory wherever the metastatic involvement is indeterminate or questionable. PET CT is recommended for restaging the recurrent tumour, and differentiating the treatment changes from recurrence in vaginal carcinomas. In cases of vaginal sarcomas, it is used for grading, staging and follow-up imaging. MRI is the main investigation for evaluation of vaginal masses and for both staging and surveillance. Patients are requested to be fasting for at least 4 hours to limit bowel motility and to empty the bladder 1 hour before the study to achieve moderate distention of the bladder. Use of antispasmodic agents like Butylscopolamine 40 mg IM/IV or Glucagon 0.5–1 mg IV/IM can also be considered to reduce bowel movements. The vagina should be distended with about 60 mL of Ultrasound Gel for evaluation of vaginal lesions. The patient is imaged in supine position with phased array abdomino pelvic coil. The saturation band is usually placed anterior and superior to the field of view. T2 imaging remains the mainstay for evaluation of vaginal tumours. The basic sequences for evaluation of vagina lesions are T2 sagittal, axial, coronal and oblique axial, T1 axial and diffusion-weighted imaging in axial plane. The high-resolution oblique axial along the plane of vagina is the best sequence which demonstrates the tumour and its extent. The study may be completed by contrast injection. The sequences for contrast evaluation will include pre-T1 with fat saturation, followed by dynamic contrast injection and postcontrast T1 fat saturated acquisition. The most common clinical presentation would be painless vaginal bleeding (65%–80%) followed by vaginal discharge, pelvic pain, urinary symptoms and mass being felt in the vagina. The primary carcinoma are usually squamous cell carcinoma and accounts for about 80% of cases. They are more commonly seen in the upper third in the posterior wall. It is associated with HPV and about 30% of women also have history or associated intraepithelial and invasive cancers of cervix and vulva. About a third of patients present with lymph nodal metastasis in the pelvis or inguinal region at the time of clinical presentation. Adenocarcinoma accounts for only 9% of primary vaginal malignancies, and they are usually seen in the anterior wall of the upper third of the vagina. They affect younger age group (14–21 years) and arise from the lesions such as endometrial deposits and the vaginal adenosis. About two-thirds of the cases have exposure to Diethylstilbestrol to their mothers. When seen in older women, they are usually clear cell carcinomas. Staging of vaginal carcinoma with MRI parallels clinical FIGO staging (Figs 11.19.2.2–11.19.2.4). The tumour is best seen on T2-weighted sequences where it is seen as an intermediate signal (higher than muscle and lower than fat). Adenocarcinomas typically exhibit high T2 signal. Because of the signal on T2, the tumour is well delineated from the vaginal wall which displays low signal intensity. When the tumour is limited to vagina, it is difficult to be seen on T1 sequences unless it causes a contour abnormality as the tumour will be isointense on T1. Stage I tumours are those which are either seen as mass/plaque like thickening but will be limited to vagina and will be diagnosed if the hypointense T2 signal of the vaginal wall is preserved (Fig. 11.19.2.5). When the tumour disrupts this hypointense layer and extends into the paravaginal fat, the staging becomes Stage II (Fig. 11.19.2.6). The loss of normal signal of the vaginal wall should be looked at all three orthogonal planes to identify subtle loss of the signal which is the important finding which upstages the tumour.
11.19: Vagina
Introduction
Classification of vaginal cysts
True Cyst
Vaginal Cyst Mimics
Complications of vaginal cysts
Müllerian cysts
Gartner duct cyst

Bartholin gland cyst
Bartholin gland abscess
Skene gland cyst

Urethral diverticulum
Introduction
Vaginal anatomy
Blood supply
Lymphatic drainage
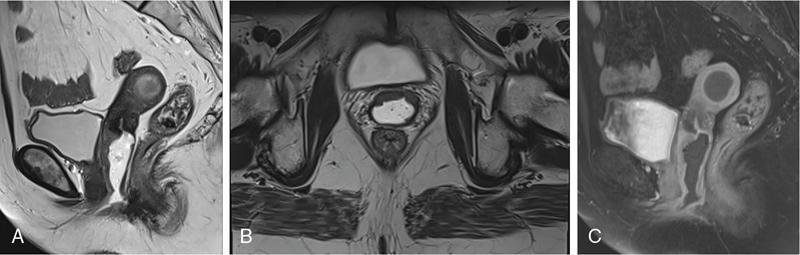
Imaging anatomy
Imaging technique
Primary vaginal carcinoma
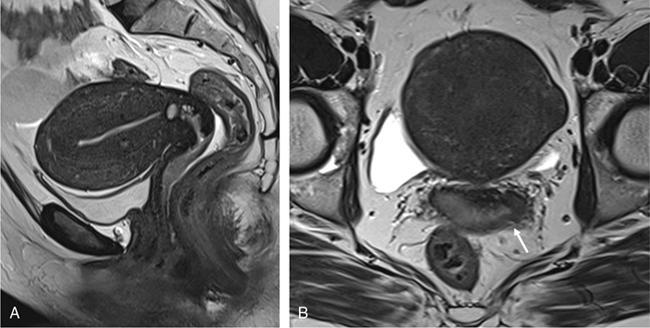
MR imaging and staging
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


